
 Submit Manuscript
Submit Manuscript
Case Report | Open Access
Robot-Assisted Adrenalectomy for a Giant Adrenal Myelolipoma: One of the Largest Tumors Removed by a Minimally Invasive Approach
Avishek Mandal1, Shikhar Chohan2, Neha K Madan2, Puneeth Medapati1, Rohan Nautiyal1, Niraj Kumar1, Pawan Vasudeva1
1Department of Urology and Renal Transplant, Vardhaman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
2Department of Pathology, Vardhaman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
Correspondence: Shikhar Chohan (Department of Pathology, Vardhaman Mahavir Medical College and Safdarjung Hospital, New Delhi, India; Email: shikhar.chohan1993@gmail.com).
Annals of Urologic Oncology 2026, 9: 3. https://doi.org/10.32948/auo.2026.03.28
Received: 08 Mar 2026 | Accepted: 08 May 2026 | Published online: 28 May 2026
Case presentation A 36-year-old woman of South Asian ethnicity presented with mild, recurrent right flank pain for 8 months. Imaging revealed a right adrenal mass (10.5 × 10.8 × 12.2 cm), which was consistent with myelolipoma. She underwent robot-assisted laparoscopic adrenalectomy using the Da Vinci Xi platform. The tumor, which closely abutted the hepatic vein, was successfully removed without complications. Final pathology confirmed a myelolipoma measuring 18.2 × 13.5 × 5.5 cm and weighing 1030 grams—one of the largest such tumor reported to have been removed robotically.
Conclusions This case highlights the feasibility and safety of robotic adrenalectomy for giant adrenal tumors in experienced hands. It sets a precedent for managing such large tumors minimally invasively and expands the scope of robotic surgery in adrenal pathology.
Key words Adrenal myelolipoma, robotic adrenalectomy, giant adrenal tumor, minimally invasive surgery, case report
The patient was positioned in a left lateral decubitus position. A standard four-port robotic configuration was used with the Da Vinci Xi system (Figure 2). Robot-assisted laparoscopic right adrenalectomy was performed. Following mobilization of the liver by dividing the right triangular and falciform ligaments, careful dissection was carried out to identify and control the adrenal vein and its tributaries draining into the inferior vena cava (IVC). The tumor was well encapsulated and closely abutted the hepatic vein, requiring meticulous dissection to avoid vascular injury (Figure 3A–D). The mass was mobilized from surrounding structures without capsular disruption and retrieved using an endoscopic retrieval bag to prevent spillage. The estimated blood loss was 200 mL, total operative time was 230 minutes, and robotic console time was 174 minutes.
The patient had an uneventful postoperative recovery and was discharged on day 3.
Gross pathology revealed a tumor measuring 18.2 × 13.5 × 5.5 cm and weighing 1030 grams. Histopathological examination confirmed the diagnosis of adrenal myelolipoma, which was composed of mature adipose tissue with interspersed hematopoietic elements and no signs of malignancy (Figure 4A–C).
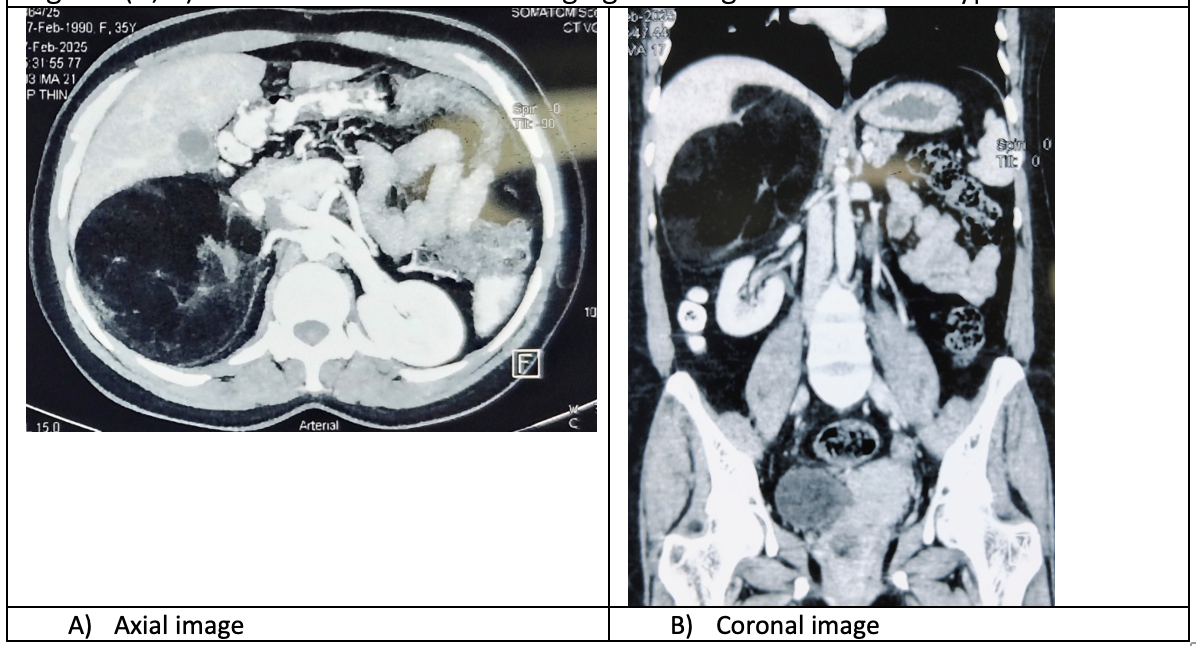 Figure 1. Contrast-enhanced CT showing a well-defined hypodense adrenal mass. (A) Axial view; (B) Coronal view.
Figure 1. Contrast-enhanced CT showing a well-defined hypodense adrenal mass. (A) Axial view; (B) Coronal view.
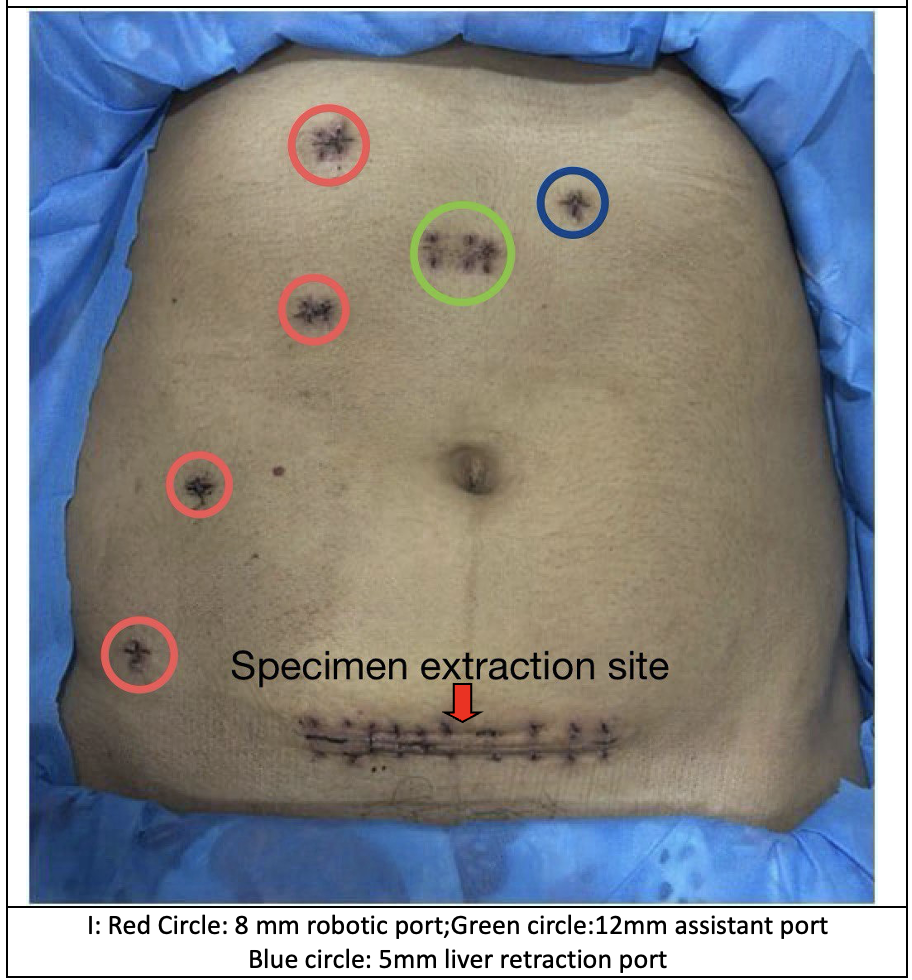 Figure 2. Port placement and specimen extraction site following robot-assisted right adrenalectomy. (A) Red circles indicate 8 mm robotic ports; (B) Green circle indicates the 12 mm assistant port; (C) Blue circle indicates the 5 mm liver retraction port. The lower transverse incision (arrow) marks the specimen extraction site.
Figure 2. Port placement and specimen extraction site following robot-assisted right adrenalectomy. (A) Red circles indicate 8 mm robotic ports; (B) Green circle indicates the 12 mm assistant port; (C) Blue circle indicates the 5 mm liver retraction port. The lower transverse incision (arrow) marks the specimen extraction site.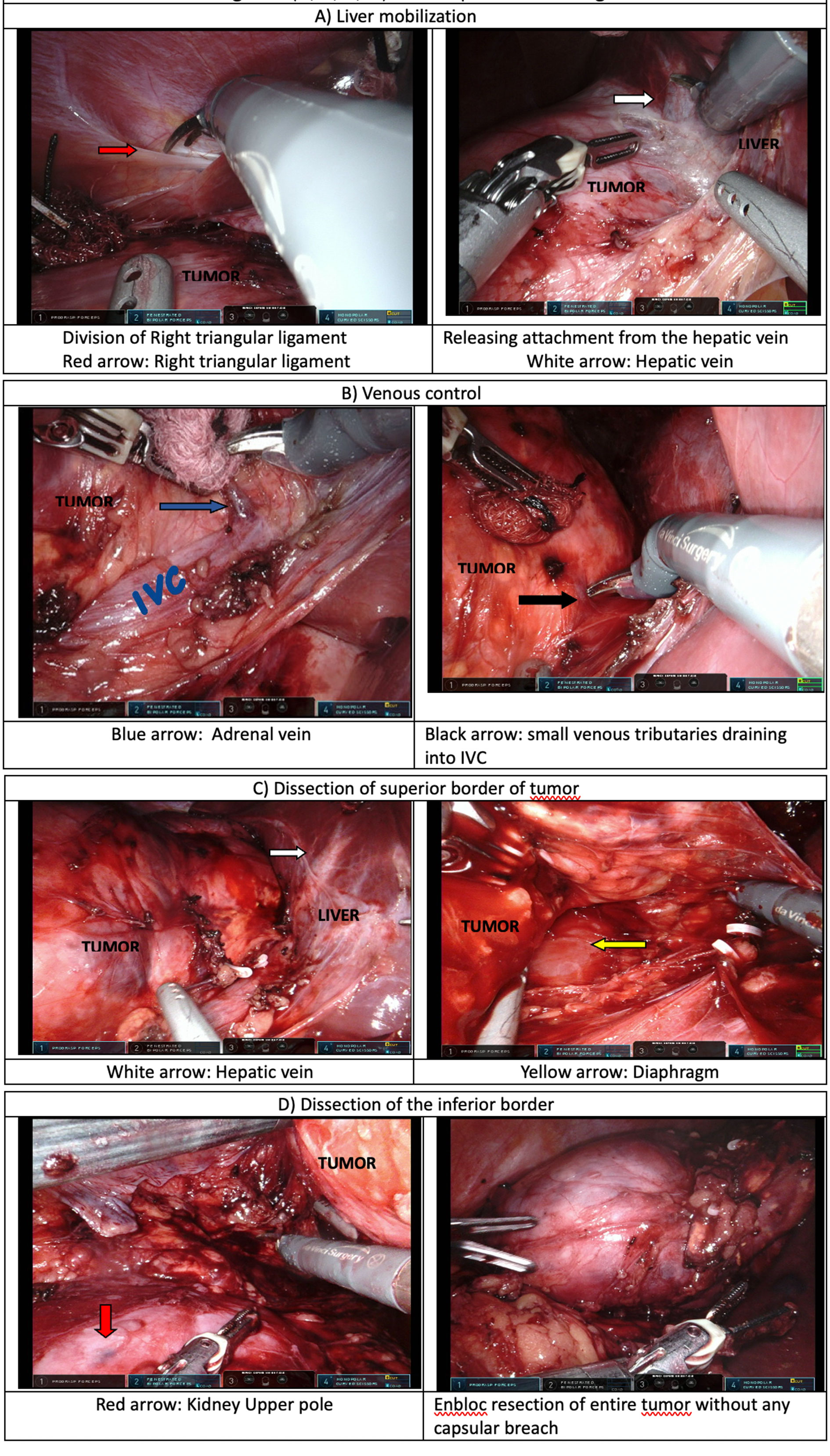 Figure 3. Intraoperative steps of robot-assisted adrenalectomy. (A) Liver mobilization; (B) Venous control; (C) Dissection of the superior border of the tumor; (D) Dissection of the inferior border of the tumor.
Figure 3. Intraoperative steps of robot-assisted adrenalectomy. (A) Liver mobilization; (B) Venous control; (C) Dissection of the superior border of the tumor; (D) Dissection of the inferior border of the tumor.
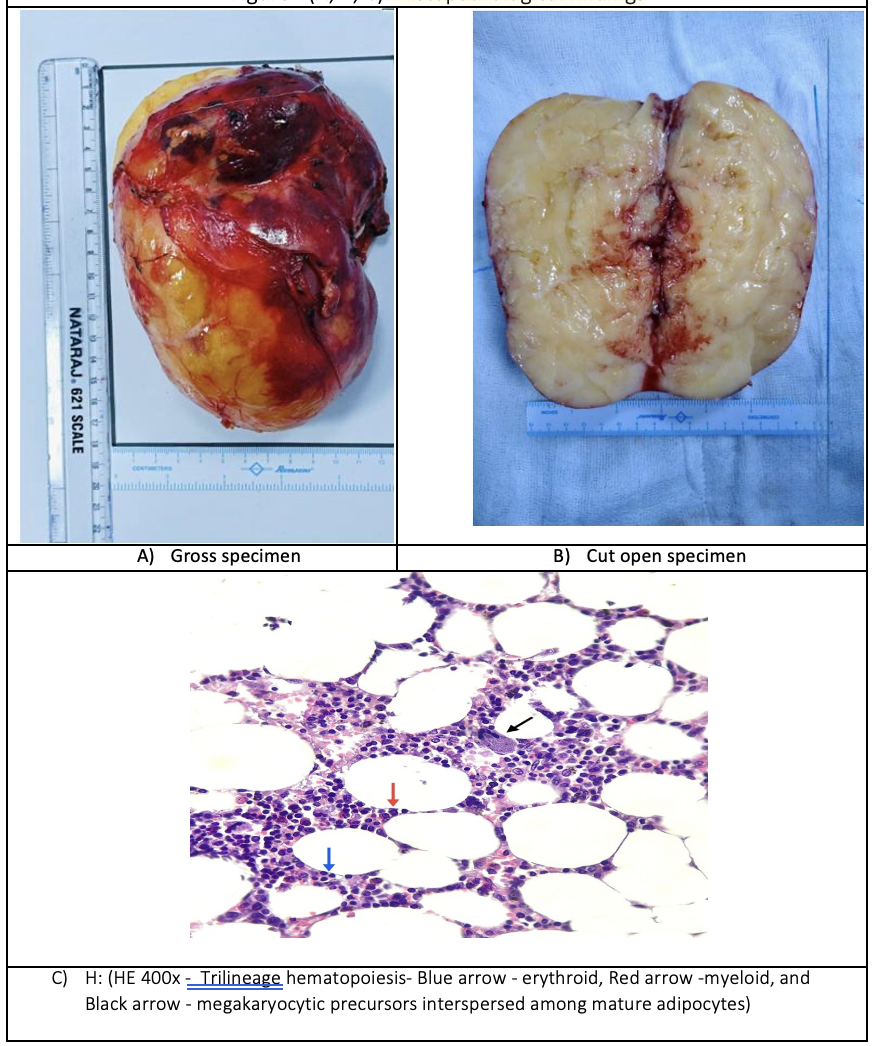 Figure 4. Histopathological features of adrenal myelolipoma. (A) Gross specimen; (B) Cut surface of the tumor; (C) Hematoxylin and eosin stain (×400) showing trilineage hematopoiesis (blue arrow: erythroid, red arrow: myeloid, black arrow: megakaryocytic precursors) admixed with mature adipocytes.
Figure 4. Histopathological features of adrenal myelolipoma. (A) Gross specimen; (B) Cut surface of the tumor; (C) Hematoxylin and eosin stain (×400) showing trilineage hematopoiesis (blue arrow: erythroid, red arrow: myeloid, black arrow: megakaryocytic precursors) admixed with mature adipocytes.
With increasing experience, minimally invasive approaches, including laparoscopic and robotic adrenalectomy, have been successfully applied to larger adrenal tumors. While an upper size limit of approximately 10–12 cm has been suggested for laparoscopic adrenalectomy, this threshold remains less clearly defined for robotic surgery [2, 3]. Tumor size can pose technical challenges by limiting visualization and instrument maneuverability, thereby increasing the risk of capsular rupture and incomplete resection. However, evidence suggests that size alone should not be considered an absolute contraindication, and the absence of local invasion on preoperative imaging remains the most important factor in selecting a minimally invasive approach [4].
Robotic adrenalectomy offers several advantages over conventional laparoscopy, including enhanced dexterity, three-dimensional visualization, and improved instrument stability. The use of the fourth robotic arm provides consistent retraction and improved exposure, facilitating meticulous dissection around critical vascular structures. Previous studies have reported that for adrenal tumors larger than 5–6 cm, robotic adrenalectomy may be associated with shorter operative time, reduced blood loss, and lower conversion rates compared with laparoscopy [5, 6].
Surgeon experience plays a crucial role in determining the feasibility of a robotic approach for large adrenal tumors. With adequate expertise, en bloc tumor resection can be achieved safely while preserving surrounding structures. Recent reports have demonstrated successful robotic adrenalectomy for tumors measuring up to 15–17 cm [7, 8]. This case adds to the growing body of evidence supporting the feasibility of robotic surgery in large adrenal tumors.
In our case, preoperative CT imaging reliably suggested myelolipoma based on the presence of macroscopic fat, and no local invasion was identified, allowing for a minimally invasive approach. However, imaging may underestimate tumor size, as previously reported, which was also observed in our case [9].
The final resected specimen measured 18.2 × 13.5 × 5.5 cm and represents one of the largest adrenal tumors removed robotically in the literature.
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Availability of data and materials
Not applicable.
Conflict of interests
The authors declare that they have no competing interests.
Funding
No funding was received.
Authors' contributions
AM: Conceptualization, Data curation, Writing – original draft.
PM: Conceptualization, Data curation.
SC: Histopathological analysis, microscopy imaging, writing – review and editing, corresponding author.
NKM: Histopathological analysis, Writing – review & editing.
RN: Writing – review & editing.
NK: Surgical supervision, Writing – review & editing.
PV: Surgical procedure, Resources, Final approval of manuscript.
Acknowledgments
Not applicable.
- Bokhari MR, Zulfiqar H, Garla VV: Adrenal Myelolipoma. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
- Henry JF, Sebag F, Iacobone M: Results of laparoscopic adrenalectomy for large and potentially malignant tumors. World J Surg 2002, 26(8): 1043-1047.
- MacGillivray DC, Whalen GF, Malchoff CD, Oppenheim DS, Shichman SJ: Laparoscopic resection of large adrenal tumors. Ann Surg Oncol 2002, 9(5): 480-485.
- Varghese B, Moinuddin Z, Augustine T: Laparoscopic approaches to adrenalectomy for large adrenal tumours: A systematic review. Laparosc Surg 2022, 6: 38.
- Agcaoglu O, Aliyev S, Karabulut K, Mitchell J, Siperstein A, Berber E: Robotic versus laparoscopic resection of large adrenal tumors. Ann Surg Oncol 2012, 19(7): 2288-2294.
- Morelli L, Tartaglia D, Bronzoni J, Palmeri M, Guadagni S, Di Franco G, Gennai A, Bianchini M, Bastiani L, Moglia A, et al: Robotic assisted versus pure laparoscopic surgery of the adrenal glands: A case-control study comparing surgical techniques. Langenbecks Arch Surg 2016, 401(7): 999-1006.
- Shah P, Ragavan N, Bhat S, Dholakiya K: Case report: Robot-assisted laparoscopic excision of giant ganglioneuroma of the adrenal gland. J Robot Surg 2018, 12(3): 553-555.
- Cochetti G, Paladini A, Boni A, Silvi E, Tiezzi A, De Vermandois JAR, Mearini E: Robotic treatment of giant adrenal myelolipoma: A case report and review of the literature. Mol Clin Oncol 2019, 10(5): 492-496.
- Lau H, Lo CY, Lam KY: Surgical implications of underestimation of adrenal tumor size by computed tomography. Br J Surg 1999, 86(3): 385-387.
Annals of urologic oncology
p-ISSN: 2617-7765, e-ISSN: 2617-7773
 Copyright © Ann Urol Oncol. This work is licensed under a Creative Commons Attribution-NonCommercial-No Derivatives 4.0 International (CC BY-NC-ND 4.0) License.
Copyright © Ann Urol Oncol. This work is licensed under a Creative Commons Attribution-NonCommercial-No Derivatives 4.0 International (CC BY-NC-ND 4.0) License.