
 Submit Manuscript
Submit Manuscript
Research Article | Open Access
68Ga-PSMA PET/CT-avid Tumour Volume: A Potential Prognostic Biomarker in Metastatic Hormone Sensitive Prostate Cancer
Greta Beale1, Alexander Yuile1, Wai-Hoong Chan1, Joseph Chan2, Andrew Kneebone2, George Hruby2, Thomas Eade2, Alexander Guminski1, Adrian Lee1, Edward Hsiao3, Madeleine Tilley1, David L Chan1, 4
1Department of Medical Oncology, Royal North Shore Hospital, Reserve Rd, St. Leonards, NSW, Australia.
2Department of Radiation Oncology, Royal North Shore Hospital, Reserve Rd, St. Leonards, NSW, Australia.
3Department of Nuclear Medicine, Royal North Shore Hospital, Reserve Rd, St. Leonards, NSW, Australia.
4Northern Clinical School, Faculty of Medicine and Health, University of Sydney, NSW, Australia.
Correspondence: David L Chan (Department of Medical Oncology, Royal North Shore Hospital, Reserve Rd, St. Leonards, NSW, Australia; Email: David.chan@sydney.edu.au).
Annals of Urologic Oncology 2026, 9: 4. https://doi.org/10.32948/auo.2026.04.06
Received: 11 Feb 2026 | Accepted: 06 Apr 2026 | Published online: 28 Jun 2026
Methods We retrospectively reviewed patients with de novo metastatic prostate cancer undergoing baseline PSMA PET/CT at Royal North Shore Hospital between 2014-2019. TTV was quantified using a standardized Standard Uptake Value (SUV) threshold, and patients were stratified by median TTV. Associations between TTV, progression-free survival (PFS), and overall survival (OS) were assessed using Kaplan–Meier and Cox regression analyses.
Results Fifty-nine patients were included in the study. Patients in the high-TTV group demonstrated reduced OS but no significant difference in PFS. Higher PSMA-derived TTV correlated with increased prostate-specific antigen (PSA) at diagnosis and higher rates of skeletal related events. Higher SUVmax was not associated with longer PFS or OS, nor was it associated with increased skeletal related events.
Conclusion Baseline PSMA PET/CT-derived tumour volume is an independent prognostic biomarker in metastatic hormone-sensitive prostate cancer, associated with inferior overall survival. Incorporating TTV into existing risk models may refine patient selection for treatment intensification.
Key words: prostate, PSMA, tumour volumes, prognostic biomarker, hormone sensitive
PSMA PET Scans have also been increasingly used to guide the use of radiopeptide therapies such as lutetium-177 (177Lu)-PSMA-617. The VISION trial showed that this novel treatment improved overall and progression-free survival in patients with metastatic castrate resistant prostate cancer [4]. As PSMA avidity is required for effective delivery and efficacy of 177Lu-PSMA, PSMA PET/CT scans will be increasingly employed to select patients for this exciting therapy.
There has been some published data for patients with metastatic castrate resistant prostate cancer (mCRPC) examining the role of total tumour volumes (TV) in PSMA PET/CT. Higher PSMA-TV was associated with poorer overall survival (OS) in patients receiving 177Lu-PSMA [5], and decreased OS and progression-free survival (PFS) for those treated with cabazitaxel chemotherapy [6-7]. Similarly, a substudy of ENZA-p, which looked at Lu-PSMA-617 plus enzalutamide in patients with mCRPC demonstrated that higher baseline PSMA-TV was associated with poorer overall survival [8]. There is, however, little data regarding the prognostic correlation between tumour volumes and outcomes in the setting of metastatic hormone sensitive prostate cancer(mHSPC), as well as its relationship to established prognostic markers such as the Gleason score and PSA. Given the evolving landscape of treatment for metastatic prostate cancer including novel anti-androgen therapies and chemotherapy in the upfront setting for high-risk hormone-sensitive metastatic patients, examining this cohort and being able to accurately assess risk has become more relevant than ever before.
We therefore sought to investigate the role of PSMA PET scans as a prognostic biomarker in patients with metastatic hormone sensitive prostate cancer, with a particular focus on the relationship between parameters such as tumour volume and SUVmax and outcome measures such as progression free survival (PFS) and overall survival (OS), which may help guide treatment decisions and individualization of systemic therapy choice.
PET/CT images were acquired on a scanner with Time-of-Flight capabilities and extended axial field of view (Biograph mCT.S/64 PET/CT, Siemens Healthcare, Hoffman Estates, USA). Injection of [68Ga] Ga-PSMA-11 at a dosage of 200–250 MBq was followed 60 minutes later by PET/CT acquisition.
Images were analysed using MIM software (version 6.8.3) applying a flat SUV threshold of 4 using a semi-automated algorithm with removal of areas of false positive avidity (e.g. bladder). These contours were subsequently reviewed by expert nuclear medicine physicians with >10 years expertise to ensure veracity of measurements. Following finalization of contours, PSMA avid tumour burden (total, primary, metastatic) was collected along with SUVmax/SUVmean.
Relevant clinicopathologic variables including age, sites of metastatic disease, baseline PSA and Gleason score, as well as clinical outcomes (progression-free and overall survival) were collected through retrospective chart review.
The primary end point was progression-free survival (PFS), with secondary end points being overall survival (OS) and time to first skeletal related event (TSRE). Both PFS and OS were censored at time of last follow-up, 9 years and 6 months. As per standard practice, progression-free survival was judged as time to a composite of radiological progression, initiation of new systemic therapy, a rise in PSA of >2 ng/mL confirmed by two tests a minimum of two weeks apart, or death. Overall survival was defined as time from treatment initiation to death from any cause. Patients were censored at date of last known follow-up where relevant. Skeletal related events were defined as: pathological fracture, spinal cord compression, necessity for radiation to bone for either pain or impending fracture, or surgery to bone.
Clinicopathological variables were presented descriptively. The patient cohort was dichotomised by median total PSMA-avid tumour volume, and Gleason score (6-7 vs 8-10), PFS, OS and TSRE were compared between such cohorts using the log-rank test.
This study received ethical approval from the NSLHD HREC, approval number 2020/ETH0059.
The median PSMA-avid tumour volume (TV) was 13.8 mL (range, 0.27-479.3), and the median SUVmax of overall tumour burden was 27.7 (range, 4.6-98.9). Patients were dichotomized into high- and low-volume groups using the median TV cutoff (Figure 1). Median PFS did not differ significantly between groups (26.5 vs 43.0 months; HR, 0.59; 95% CI, 0.31-1.14; p = 0.118). In contrast, median OS was significantly shorter in the high-TV group than in the low-TV group (56.6 vs 82.3 months; HR, 0.29; 95% CI, 0.11-0.77; p = 0.013) (Figure 2).
There was no difference in overall survival between patients in cohort 1 (ADT alone) and those in cohort 2 (ADT with additional therapy, either chemotherapy or targeted therapy) (median OS 66.6mo vs NR), HR 0.62 95% CI 0.0-1.79, p = 0.38). OS was numerically higher for patients on ADT alone, likely reflecting the more indolent biology of this group resulting in their selection for ADT alone. There was also no significant difference when comparing patients with ADT alone and those who had ADT + targeted therapy (i.e. excluding those who had ADT + chemotherapy) - (median OS 66.6mo vs 41.6mo, HR 0.62, 95% CI 0.19-2.02). Detailed analyses for overall survival by univariate analyses are shown in Table 2. Multivariate analyses were not performed due to the small size of the patient cohort.
Finally, we investigated the prognostic value of SUVmax in our cohort, appreciated the relative lack of data linking SUVmax to survival outcomes to date. SUVmax on PSMA PET was not significantly associated with PFS (HR, 1.01; 95% CI, 0.99-1.02; p = 0.264), OS (HR, 1.02; 95% CI, 0.99-1.04; p = 0.120), or skeletal-related events (SREs) (HR, 1.01; 95% CI, 0.99-1.04; p = 0.260).
As expected, patients with Gleason score 6-7 disease had improved survival compared with those with Gleason score 8-10. Median OS was 82.3 vs 64.8 months (HR, 0.35; 95% CI, 0.12-0.93; p = 0.036), and median PFS was 57.0 vs 21.6 months (HR, 0.34; 95% CI, 0.17-0.64; p = 0.002). Tumour burden was also significantly lower in the Gleason score 6-7 cohort (mean, 32.7 vs 77.7 mL; p = 0.030).
Twelve skeletal-related events occurred: 8 patients required radiotherapy for painful or unstable bony lesions, 2 sustained pathological fractures, 1 developed spinal cord compression, and 1 underwent surgery for pain or impending cord compression. Time to skeletal-related event (TSRE) was shorter in the high-TV group compared with the low-TV group (HR, 4.6; 95% CI, 1.33-15.97; p = 0.030), although the median TSRE was not reached in either cohort.
|
Table 1. Clinicopathologic characteristics of the cohort (n = 59). |
|
|
Characteristic |
Value |
|
Age, y |
Median 72 (range, 48-88) |
|
Baseline PSA, µg/L |
Median 7.9 (range, 0.19-282) |
|
Gleason score, n (%) |
|
|
6-7 |
24 (41) |
|
8-10 |
32 (54) |
|
Unknown |
3 (5) |
|
Systemic therapy, n (%) |
|
|
ADT alone |
39 (66) |
|
ADT + enzalutamide |
11 (19) |
|
ADT + abiraterone |
6 (10) |
|
ADT + docetaxel |
2 (3) |
|
ADT + other |
1 (2) |
|
PSMA-avid tumour volume, mL |
Median 13.8 (range, 0.27-479.3) |
|
SUVmax of overall tumour burden |
Median 27.7 (range, 4.6-98.9) |
|
ADT = androgen deprivation therapy; CT = computed tomography; mHSPC = metastatic hormone-sensitive prostate cancer; PSMA = prostate-specific membrane antigen. |
|
|
Table 2. Univariate analysis for overall survival. |
||
|
Category |
Median OS (months) |
Hazard Ratio (HR) |
|
Cohort 1 (ADT + Additional Tx) |
Not reached |
|
|
Cohort 2 (ADT alone)
|
66.6 |
HR 0.65 (95% CI 0.23-1.8); p=0.38 |
|
Gleason Score ≥8 |
64.8 |
|
|
Gleason Score ≤7 |
82.3 |
HR 0.35 (95% CI 0.12-0.93); p=0.036 |
|
High Tumour Volume |
56.6 |
|
|
Low Tumour Volume |
82.3 |
HR 0.29 (95% CI 0.11-0.77); p=0.013 |
|
ADT = androgen deprivation therapy; CT = computed tomography; mHSPC = metastatic hormone-sensitive prostate cancer; PSMA = prostate-specific membrane antigen. |
||
|
Table 3. Definitions of high-volume and high-risk disease in landmark mPC trials. |
||
|
Study |
Setting and treatment |
Definition of high volume / high risk disease |
|
CHAARTED |
Metastatic hormone-sensitive prostate cancer; docetaxel + ADT |
Presence of visceral metastases and/or ≥4 bone metastases with ≥1 beyond the vertebral column and pelvis |
|
LATITUDE |
Metastatic hormone-sensitive prostate cancer; abiraterone + prednisone + ADT |
High risk: ≥2 of the following— |
|
ARASENS |
Metastatic hormone-sensitive prostate cancer; darolutamide + docetaxel + ADT |
High volume: Visceral metastases and/or ≥4 bone metastases with ≥1 beyond the vertebral column/pelvis |
|
Proposed definition |
|
High PSMA tumour volume cutoff ≥14 mL |
|
ADT = androgen deprivation therapy; CT = computed tomography; mHSPC = metastatic hormone-sensitive prostate cancer; PSMA = prostate-specific membrane antigen.
|
||
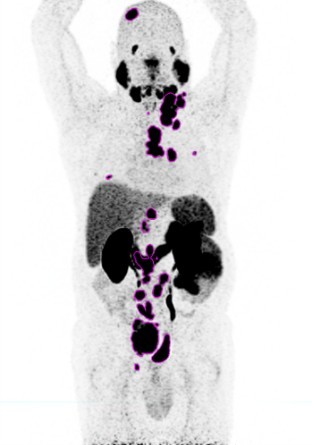 Figure 1. Indicative [68Ga] Ga-PSMA-11 PET/CT image, maximal intensity projection (PSMA-avid lesions outlined in blue).
Figure 1. Indicative [68Ga] Ga-PSMA-11 PET/CT image, maximal intensity projection (PSMA-avid lesions outlined in blue).
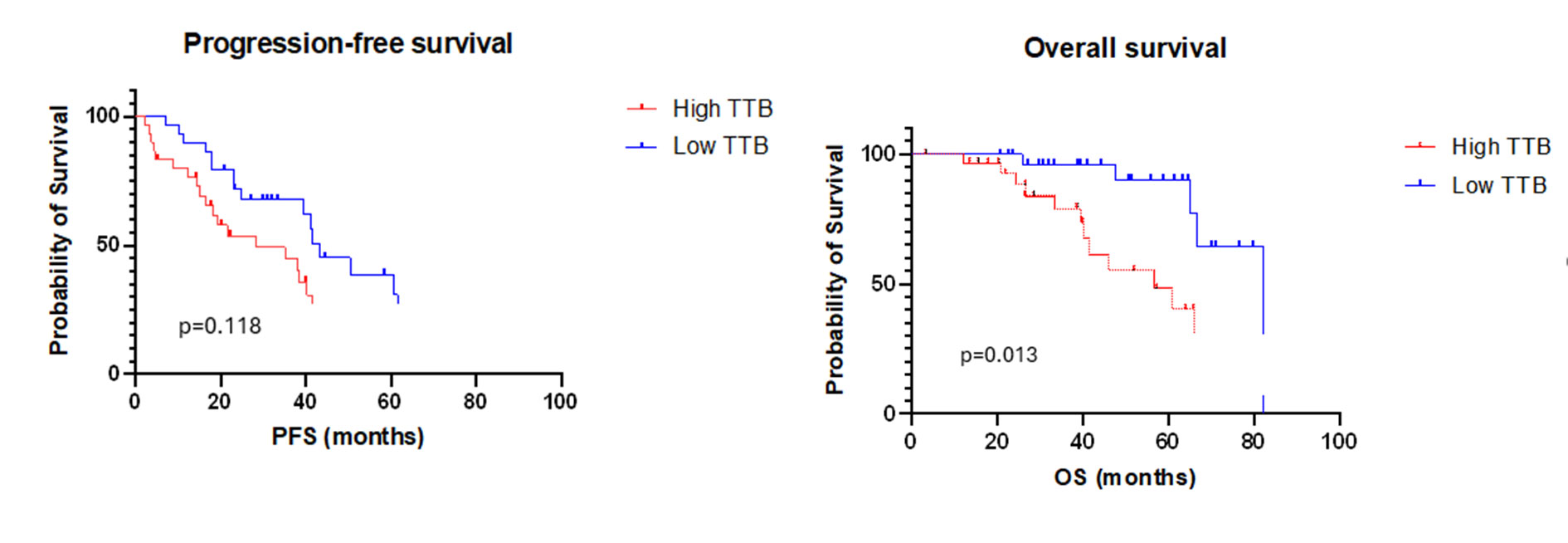 Figure 2. PFS and OS in the high-TV group and the low-TV group.
Figure 2. PFS and OS in the high-TV group and the low-TV group.
The median tumour volume of 14 mL in the current study was used to dichotomize our study cohort, and a statistically significant difference in overall survival was observed between the high TV and low TV cohorts. We do note that studies examining the prognostic and predictive value of PSMA-TTV in the metastatic castrate resistant setting had much higher median tumour volumes [13, 16]. Interestingly, whilst OS was significantly lower in the high TV group compared to the low TV group, the difference in PFS between the two groups was not statistically significant. The finding with regards to OS is consistent with existing literature [5-6], and the lack of significance with regard PFS may potentially be explained by the heterogeneity of patients included in the current study, or the small cohort. This finding may also potentially suggest that treatment is effective in early lower volume disease but less so in higher volume disease Other variables which were considered in our analysis also need to be taken into account, for example the difference in overall survival between the different treatment arms of Cohort 1 and Cohort 2, as well as OS differences by Gleeson score. Of note, 1 patient with histological evidence of neuroendocrine differentiation was included in our study, which was an exclusion criteria for LATITUDE.
Interestingly the SUVmax on PSMA PET was not significantly associated with improved survival or skeletal related events. This is concordant with prior studies that demonstrated a statistically significant correlation with PSA levels as a surrogate marker of tumour burden, whereas SUVmax and SUVmean did not correlate to OS in early stage or biochemically recurrant disease [14-15]. The relationship between PSMA PET scan as potential biomarker and other existing biomarkers needs to be further explored in the metastatic hormone sensitive setting.
It is also notable that there is no widely accepted voluming method for PSMA PET. Contouring using both relative (percentages of SUVmax) and absolute (flat) thresholds have been investigated. Whilst prior studies have suggested SUVmax cutoffs of 5.30 [13] and 3 [16], we adopted a SUV cutoff of 4 based on review of locally acquired imaging to strike a balance between identifying disease effectively and minimising identification of physiological uptake. The European Association of Nuclear Medicine (EANM) recommends the use of percentage-based thresholding of SUVmax for assessment of tumour volume in 18F-FDG PET/CT [17], however there is no recommendation to date regarding contouring of 68Ga-PSMA PET/CT imaging. Studies have demonstrated the limitations of both relative and absolute thresholding [18-19]. We opted for a flat cutoff in the current study in an aim to establish a time-efficient, reproducible thresholding approach. There is a pressing need to define the best tumour voluming method to provide a quantitative imaging biomarker that can be used for prognostication, as well as to measure response.
We adopted an innovative semi-automated workflow in the current study, with contour verification by an experienced nuclear medicine physician to confirm accuracy. This paves the way to efficient generation of tumour volumes for potential clinical translation, as well as annotation of datasets for large-scale radiomic analysis and training of machine learning models. There has however been prior studies examining the accuracy of semi- automated methods for analysing PSMA PET tumour volumes with concern between variability between difference platforms which may limit clinical comparibility [20-22]. It has been noted that assessment of volumetric parameters was time and labour intensive [14], again emphasizing the importance of generating an accurate and reproducible semi-automatic voluming method.
The strengths in this study lie in the robust imaging analysis which utilised semi-automated software to improve efficiency. To our knowledge it is the first data looking at prostate cancer in the metastatic castrate sensitive setting, and complements the existing literature on tumour volumes in more advanced disease, as well as that published regarding lutetium therapy. We acknowledge the relatively small numbers in this single centre, retrospective study. There is a need to investigate the prognostic value of tumour volumes in an expanded multicentre retrospective study, as well as validation of our findings in prospective clinical trial settings to translate it to clinical practice. Prospective studies will also allow for the protocolised collection of prognostic variables such as performance status, PSA and histopathological variables.
GB drafted the manuscript and analysed the data, AY assisted with drafting the manuscript and collecting data, DC assisted with drafting the manuscript, statistical analysis and developed the design of the study. MT and WHC assisted with data collection. EH analysed images. JC, TE, GH, AK, AG and AL assisted with study design and coordination, All authors read and approved the final manuscript.
Competing interests
All authors declare no competing interests.
Acknowledgement
None.
- Australian Institute of Health and Welfare. Cancer [Internet]. Available from: https://www.aihw.gov.au/reports/australias-health/cancer. Accessed 2025 May 3.
- Tarr GP, Kashyap P, Dixit DD, Williams AK, Koya MP, Lim R: Utility of Ga68 prostate-specific membrane antigen positron-emission tomography for pre-operative staging of high-risk prostate cancer in a prospective cohort. J Med Imaging Radiat Oncol 2020, 64(1): 78-86.
- Roberts MJ, Roberts NA, Pelecanos A, Yaxley JW, Harley SJD, Siriwardana AR, Cullen K, Prior M, Lindsay K, Vela I, et al: A prospective, multi-centre trial of PSMA-PET compared to FDG-PET for staging of newly diagnosed high-risk prostate cancer. EJNMMI Res 2025, 15(1): 92.
- Sartor O, de Bono J, Chi KN, Fizazi K, Herrmann K, Rahbar K, Tagawa ST, Nordquist LT, Vaishampayan N, El-Haddad G, et al: Lutetium-177–PSMA-617 for metastatic castration-resistant prostate cancer. N Engl J Med 2021, 385(12): 1091-1103.
- Hartrampf PE, Hüttmann T, Seitz AK, Kübler H, Serfling SE, Schlötelburg W, Michalski K, Rowe SP, Pomper MG, Buck AK, et al: SUVmean on baseline [18F]PSMA-1007 PET and clinical parameters are associated with survival in prostate cancer patients scheduled for [177Lu]Lu-PSMA I&T. Eur J Nucl Med Mol Imaging 2023, 50(11): 3465-3474.
- Shagera QA, Karfis I, Sideris S, Guiot T, Woff E, Martinez-Chanza N, Roumeguere T, Gil T, Flamen P, Artigas C: Tumor volume on PSMA PET as a prognostic biomarker in prostate cancer patients treated with cabazitaxel. Clin Nucl Med 2023, 48(9): 775-780.
- Shagera QA, Artigas C, Karfis I, Critchi G, Chanza NM, Sideris S, Peltier A, Paesmans M, Gil T, Flamen P: (68)Ga-PSMA PET/CT for response assessment and outcome prediction in metastatic prostate cancer patients treated with taxane-based chemotherapy. J Nucl Med 2022, 63(8): 1191-1198.
- Emmett L, Papa N, Subramaniam S, Crumbaker M, Nguyen A, Joshua AM, Sandhu S, Weickhardt A, Lee ST, Ng S, et al: Prognostic and predictive value of baseline PSMA-PET total tumour volume and SUVmean in metastatic castration-resistant prostate cancer in ENZA-p (ANZUP1901): a substudy from a multicentre, open-label, randomised, phase 2 trial. Lancet Oncol 2025, 26(9): 1168-1177.
- Kyriakopoulos CE, Chen YH, Carducci MA, Liu G, Jarrard DF, Hahn NM, Shevrin DH, Dreicer R, Hussain M, Eisenberger M, et al: Chemohormonal therapy in metastatic hormone-sensitive prostate cancer: long-term survival analysis of the randomized phase III E3805 CHAARTED trial. J Clin Oncol 2018, 36(11): 1080-1087.
- Fizazi K, Tran N, Fein L, Matsubara N, Rodriguez-Antolin A, Alekseev BY, Özgüroğlu M, Ye D, Feyerabend S, Protheroe A, et al: Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med 2017, 377(4): 352-360.
- Hussain M, Tombal B, Saad F, Fizazi K, Sternberg CN, Crawford ED, Shore N, Kopyltsov E, Kalebasty AR, Bögemann M, et al: Darolutamide plus androgen-deprivation therapy and docetaxel in metastatic hormone-sensitive prostate cancer by disease volume and risk subgroups in the phase III ARASENS trial. J Clin Oncol 2023, 41(20): 3595-3607.
- Unterrainer LM, Hope TA, Fendler WP, Grogan T, Ndlovu H, Armstrong W, Barbato F, Benz MR, Rettig MB, Kishan AU, et al: Low- and high-volume disease in metastatic hormone-sensitive prostate cancer: from CHAARTED to PSMA PET—an international multicenter retrospective study. J Nucl Med 2025, 66(1): 54-60.
- Fan J, Xu K, Jiang Z, Gan C, Song H, Gao G, Wang G, Kang Q, Luo L, Wang Z, et al: Role of 18F-PSMA-1007 PET/CT-derived quantitative volumetric tumor parameters in cytoreductive radical prostatectomy selection for patients with low-volume metastatic hormone-sensitive prostate cancer: a retrospective study. BMC Cancer 2025, 25(1): 192.
- Schmuck S, von Klot CA, Henkenberens C, Sohns JM, Christiansen H, Wester HJ, Ross TL, Bengel FM, Derlin T: Initial experience with volumetric 68Ga-PSMA I&T PET/CT for assessment of whole-body tumor burden as a quantitative imaging biomarker in patients with prostate cancer. J Nucl Med 2017, 58(12): 1962-1968.
- Cardoza-Ochoa D, Cristancho-Rojas C, Rivera-Bravo B: Initial experience with volumetric 18F-PSMA-1007 PET/CT for assessment of whole-body tumor burden as a quantitative imaging biomarker in biochemically recurrent prostate cancer. J Nucl Med 2021, 62(Suppl 1): 1315.
- Buteau JP, Martin AJ, Emmett L, Iravani A, Sandhu S, Joshua AM, Francis RJ, Zhang AY, Scott AM, Lee ST, et al: PSMA and FDG-PET as predictive and prognostic biomarkers in patients given [177Lu]Lu-PSMA-617 versus cabazitaxel for metastatic castration-resistant prostate cancer (TheraP): a biomarker analysis from a randomised, open-label, phase 2 trial. Lancet Oncol 2022, 23(11): 1389-1397.
- Boellaard R, Delgado-Bolton R, Oyen WJ, Giammarile F, Tatsch K, Eschner W, Verzijlbergen FJ, Barrington SF, Pike LC, Weber WA, et al: FDG PET/CT: EANM procedure guidelines for tumour imaging: version 2.0. Eur J Nucl Med Mol Imaging 2015, 42(2): 328-354.
- Kim M, Seifert R, Fragemann J, Kersting D, Murray J, Jonske F, Pomykala KL, Egger J, Fendler WP, Herrmann K, et al: Evaluation of thresholding methods for the quantification of [68Ga]Ga-PSMA-11 PET molecular tumor volume and their effect on survival prediction in patients with advanced prostate cancer undergoing [177Lu]Lu-PSMA-617 radioligand therapy. Eur J Nucl Med Mol Imaging 2023, 50(7): 2196-2209.
- Jiao J, Kang F, Zhang J, Quan Z, Wen W, Zhao X, Ma S, Wu P, Yang F, Guo W, et al: Establishment and prospective validation of an SUVmax cutoff value to discriminate clinically significant prostate cancer from benign prostate diseases in patients with suspected prostate cancer by 68Ga-PSMA PET/CT: a real-world study. Theranostics 2021, 11(17): 8396-8411.
- Schmidkonz C, Cordes M, Schmidt D, Bäuerle T, Goetz TI, Beck M, Prante O, Cavallaro A, Uder M, Wullich B, et al: 68Ga-PSMA-11 PET/CT-derived metabolic parameters for determination of whole-body tumor burden and treatment response in prostate cancer. Eur J Nucl Med Mol Imaging 2018, 45(11): 1862-1872.
- Raad S, Winzer R, Apolle R, Brogsitter CC, Pretze M, Bundschuh RA, Miederer M, Hoberück S: Prognostic value of baseline PSMA PET/CT tumor volume in mCRPC: comparison of a semi-automated and an AI-based segmentation method. Research Square [Preprint] 2025, Version 1.
- Gafita A, Bieth M, Krönke M, Tetteh G, Navarro F, Wang H, Günther E, Menze B, Weber WA, Eiber M: qPSMA: semiautomatic software for whole-body tumor burden assessment in prostate cancer using 68Ga-PSMA-11 PET/CT. J Nucl Med 2019, 60(9): 1277-1283.
Annals of urologic oncology
p-ISSN: 2617-7765, e-ISSN: 2617-7773
 Copyright © Ann Urol Oncol. This work is licensed under a Creative Commons Attribution-NonCommercial-No Derivatives 4.0 International (CC BY-NC-ND 4.0) License.
Copyright © Ann Urol Oncol. This work is licensed under a Creative Commons Attribution-NonCommercial-No Derivatives 4.0 International (CC BY-NC-ND 4.0) License.