
 Submit Manuscript
Submit Manuscript
Review Article | Open Access
Advances in Illuminating Prostate Cancer with Emerging Phototherapies
Ali Usman1
1Department of Pharmacology, Boston University, Boston, MA 02215, USA.
Correspondence: Ali Usman (Department of Pharmacology, Boston University, Boston, MA 02215, USA; Email: usmanali@gmail.com).
Annals of Urologic Oncology 2025, 8(1): 21-29. https://doi.org/10.32948/auo.2025.01.29
Received: 25 Oct 2024 | Accepted: 19 Jan 2025 | Published online: 31 Jan 2025
Abstract
Prostate cancer is a worldwide health concern in men, with substantially high incidence rate and advanced metastatic disease-related mortality rates. Despite advancements in diagnostics and treatment options, conventional therapies for prostate cancer, including surgery, radiotherapy, chemotherapy and androgen deprivation therapy, face limitations such as treatment resistance, limited precision and off-target side-effects. Hence, identification and clinical translation of novel therapeutic strategies is urgently needed. In this regard, phototherapies, such as photodynamic therapy (PDT) and photothermal therapy (PTT), are emerging as promising options for addressing the challenges associated with conventional treatment options. Utilizing near-infrared (NIR) light to selectively target cancer cells, these approaches spare healthy tissues. PDT employs photosensitizers to produce reactive oxygen species, thereby stimulating anti-tumor immune responses, disrupting the tumor microvasculature and/or inducing aopotitic or necrotic cell death. In contrast, PTT leverages photothermal agents to generate localized hyperthermia, achieving effective thermal ablation of tumor cells. Recent advancements in nanoparticle technology have significantly improved the efficacy and specificity of these phototherapies. Functionalized nanoparticles, such as those targeting prostate-specific membrane antigen (PSMA), enhance the precision of therapeutic delivery, reducing systemic toxicity. Combination strategies incorporating PDT and PTT with conventional modalities, including surgery, chemotherapy and immunotherapy, have demonstrated synergistic effects, leading to better therapy sensitization. Preclinical and clinical studies underline the potential of these multimodal approaches to enhance treatment outcomes, particularly for advanced and castration-resistant prostate cancer. This review explores the recent innovations in illuminating prostate cancer with phototherapies, their combination with conventional therapies, and their clinical potential in reducing the global prostate cancer burden.
Key words prostate cancer, photodynamic therapy, photothermal therapy, targeted therapy, combination therapy
Key words prostate cancer, photodynamic therapy, photothermal therapy, targeted therapy, combination therapy
Introduction
Prostate cancer remains the most frequently diagnosed malignancy among men in over half the countries worldwide, with approximately 1.5 million new cases reported globally in 2022 [1]. The rising incidence of prostate cancer in recent years is particularly concerning, though much of this increase is likely due to improved detection methods through enhanced screening practices [2]. Despite significant advancements in prostate cancer diagnostics,195, it is the fifth leading cause of cancer-related deaths in men with advanced prostate cancer being responsible for around 400,000 deaths annually, and projections suggest this number could double by 2040 [1, 3]. The management of prostate cancer encompasses various approaches, including surgical intervention, chemotherapy, radiotherapy and immunotherapy. These traditional treatments come with their own drawbacks, including limited precision and undesirable side effects [4, 5]. In addition, many patients eventually experience disease progression, culminating in the development of androgen-independent castration-resistant prostate cancer (CRPC), which is often fatal [6]. Multiple pathways have been identified that may explain the progression to CRPC, involving both androgen receptor-dependent and androgen receptor-independent signaling mechanisms [4, 7]. Advancements in the management of Prostate cancer have led to the introduction of next-generation AR signaling inhibitors, which include drugs targeting androgen synthesis and more effective AR antagonists [8]. While these therapies can extend progression-free intervals and improve overall survival, resistance to these treatments eventually arises as well. A substantial number of patients with localized prostate cancer remain at a high risk of developing distant metastases, irrespective of prior local treatments [9]. Once metastasis occurs, androgen deprivation therapy becomes the primary systemic treatment, effectively delaying clinical progression [10]. However, despite initial responses, many patients treated with androgen deprivation therapy experience disease progression to metastatic castration resistant prostate cancer (mCRPC), during which cancer cells develop mechanisms to survive and proliferate even in the presence of castration-level testosterone [11]. At this advanced stage of disease, therapeutic options are extremely limited, and most patients experience rapid disease progression [12], underscoring the urgent need for innovative treatment strategies. In this context, phototherapies has gained attention as a promising and innovative treatment for prostate cancer, offering advantages such as higher specificity, lower invasiveness, and consistent reproducibility [13, 14]. Here, we explore the current progress in the use of phototherapies as a treatment for prostate cancer, discuss their potential combination with conventional therapies to improve treatment outcomes, and highlight the considerations to improve the efficacy of phototherapies to reduce the global prostate cancer burden.
Phototherapy
Phototherapy represents a potential avenue for cancer treatment with promising options such as photodynamic therapy (PDT) and photothermal therapy (PTT) (Figure 1) [15]. Nanoparticles are central to these therapies as they function as photosensitizers in PDT and photothermal agents in PTT [16]. Additionally, PDT and PTT utilize near-infrared (NIR) light (700–1100 nm), corresponding to a biological window optimal for maximizing tissue penetration by light. NIR is an optimal choice due to its ability to penetrate deeply into tissues while causing minimal damage to surrounding healthy tissues [17, 18]. Hence, NIR light is considered superior from other commonly used wavelengths in biomedical applications, such as ultraviolet or visible light, which tend to cause more substantial harm [19]. In addition, NIR light demonstrates greater penetration efficiency in tumor tissues compared to normal tissues. For instance, light with a wavelength of 630 nm can penetrate approximately 0.9 mm in normal brain tissue but extends to 1.6 mm in lung cancer tissue. [20]. Finally, the NIR region coincides with minimal absorption by water and biomolecules, making it particularly advantageous for phototherapy applications [21].
PDT relies on the combination of a molecular oxygen, light and photosensitizer to generate reactive oxygen species that can induce the death of tumor cells [22]. Photosensitizer molecules capture light at specific wavelengths, which triggers a process that activates them and results in the targeted elimination of abnormal cells [23]. This approach leads to tumor destruction via three primary mechanisms: activation of an immune response, disruption of the tumor vasculature, and direct cell death [22, 24]. PDT can provoke and modulate immune responses that contribute to long-term tumor control [23]. PDT can modulate the adaptive immune response, either enhancing or inhibiting it, depending on the specific treatment protocol used [25]. The oxidative damage caused by PDT can initiate an inflammatory response, resulting in the release of pro-inflammatory mediators that attract innate immune cells. These cells, in turn, activate a systemic anti-tumor immune response. Additionally, increasing evidence indicates that PDT aids in tumor cell destruction by boosting T-cell-mediated immune responses and fostering long-lasting immune memory [26]. PDT can induce the disruption of the tumor's microvasculature, leading to impaired blood supply and subsequent tumor cell death. This effect is achieved by targeting the photosensitizers to the blood vessels and using a brief drug-light interval [23]. The vascular effects of PDT can be specifically directed to the tumor and its surrounding tissues, offering significant advantages over other PDT protocols that focus on photosensitizer accumulation within tumor cells themselves [27]. In addition to programmed apoptotic cell death, PDT also induces non-programmed necrotic cell death [28, 29], that results in the release of cellular components and molecules that provoke an inflammatory response [30]. PDT has been shown to induce several non-conventional cell death pathways in cancer cells, as well such as pyroptosis, necroptosis, ferroptosis, paraptosis and parthanatos [29]. In particular, the necrosis of tumor cells and vasculature induced by PDT can also activate CD8+ cytotoxic T lymphocytes, which target and destroy tumor cells while circulating in the body for extended periods [23, 28].
PTT operates independently of oxygen and utilizes NIR laser absorbers to generate heat, enabling thermal ablation of cancer cells under NIR laser exposure [15, 16]. Photothermal agents are administered intravenously or directly into the tumor, where they accumulate at the targeted site. When exposed to light at specific wavelengths, these agents absorb the light energy, causing them to shift from their ground state to an excited singlet state. The energy is then released through vibrational relaxation, a non-radiative decay process, in which the molecules return to their ground state by transferring energy to nearby molecules [31]. The elevation of kinetic energy during PTT leads to a rise in local tissue temperatures, thereby heating the surrounding microenvironment. When tissues reach 41°C, a heat-shock response is activated. This response leads to rapid changes in gene expression to counteract heat-induced damage, primarily through the production of heat-shock proteins [32]. At 42°C, tissue damage becomes irreversible. Prolonged exposure to temperatures between 42°C and 46°C for 10 minutes leads to substantial cell death. In the 46–52°C range, rapid cell death occurs due to microvascular thrombosis and subsequent ischemia. When tissue temperatures surpass 60°C, immediate cell death results from protein denaturation and the destruction of the plasma membrane [33]. However, research has demonstrated that temperatures surpassing 49 °C predominantly induce necrotic cell death, which may lead to inflammation and promote secondary tumor growth [34]. Notably, maintaining a highly controlled temperature range of 46–49 °C has been identified as optimal for eradicating tumors [35]. Within the NIR spectrum, the NIR-I window of 750–900 nm is currently the most widely used range in PTT research. However, there is growing interest in exploring the NIR-II range (wavelengths exceeding 1000 nm) to enhance therapeutic efficacy as the longer wavelengths of the NIR-II region reduce tissue scattering and have lower photon energy, enabling even greater tissue penetration depths [36]. Overall, phototherapies offers promising avenues in limiting tumor burden through innovative and targeted approaches.
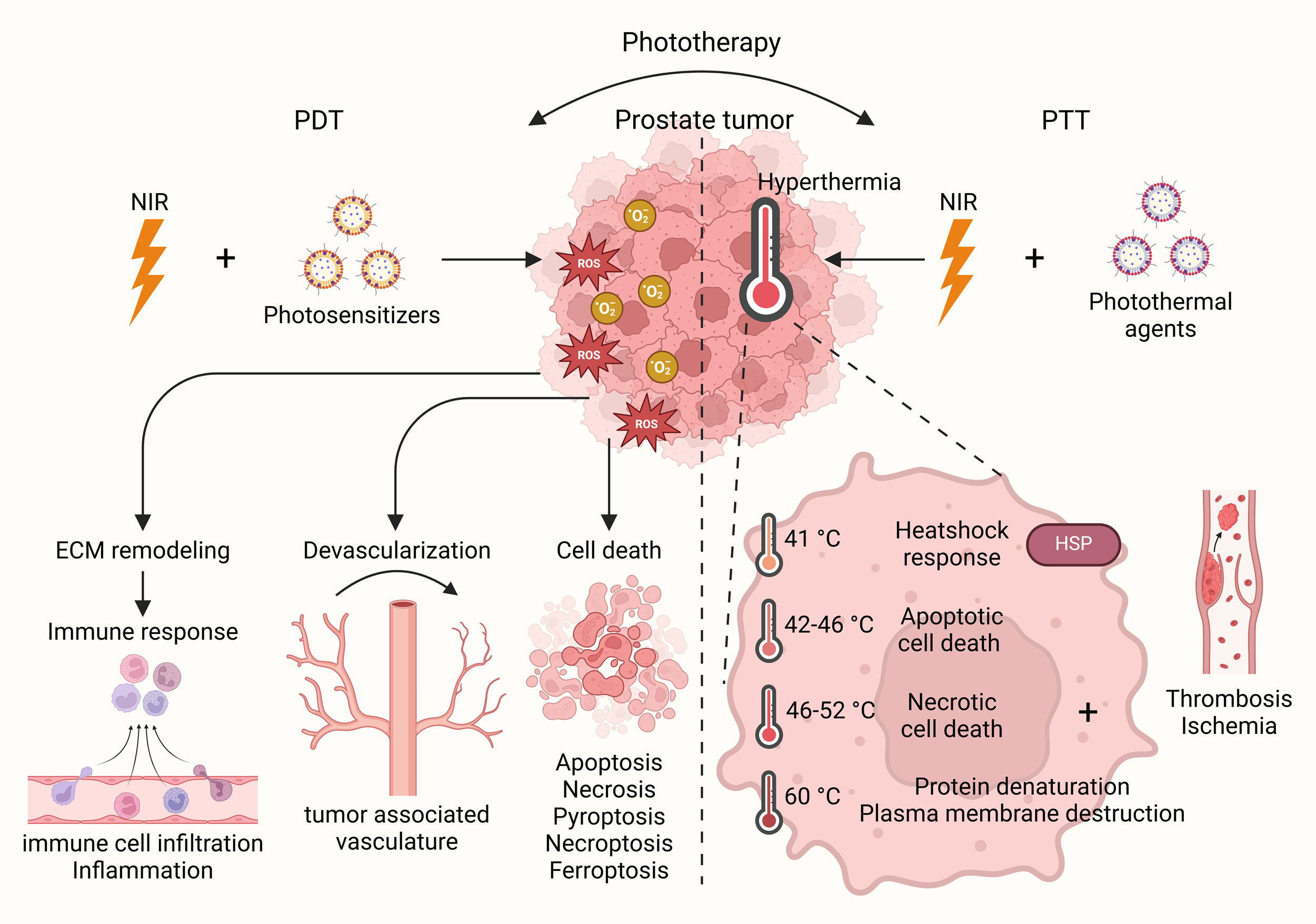 Figure 1. Phototherapy in prostate cancer. Phototherapy represents a potential avenue for cancer treatment with promising options such as PDT and PTT. Under NIR light, PDT, with the help of photosensitizers, enhances immune response, devascularization and cell death based on induction of ROS, whereas PTT, with the help of photothermal agents, induces hyperthermia leading to heatshock response and cell death in prostate cancer cells.
Figure 1. Phototherapy in prostate cancer. Phototherapy represents a potential avenue for cancer treatment with promising options such as PDT and PTT. Under NIR light, PDT, with the help of photosensitizers, enhances immune response, devascularization and cell death based on induction of ROS, whereas PTT, with the help of photothermal agents, induces hyperthermia leading to heatshock response and cell death in prostate cancer cells.
PDT relies on the combination of a molecular oxygen, light and photosensitizer to generate reactive oxygen species that can induce the death of tumor cells [22]. Photosensitizer molecules capture light at specific wavelengths, which triggers a process that activates them and results in the targeted elimination of abnormal cells [23]. This approach leads to tumor destruction via three primary mechanisms: activation of an immune response, disruption of the tumor vasculature, and direct cell death [22, 24]. PDT can provoke and modulate immune responses that contribute to long-term tumor control [23]. PDT can modulate the adaptive immune response, either enhancing or inhibiting it, depending on the specific treatment protocol used [25]. The oxidative damage caused by PDT can initiate an inflammatory response, resulting in the release of pro-inflammatory mediators that attract innate immune cells. These cells, in turn, activate a systemic anti-tumor immune response. Additionally, increasing evidence indicates that PDT aids in tumor cell destruction by boosting T-cell-mediated immune responses and fostering long-lasting immune memory [26]. PDT can induce the disruption of the tumor's microvasculature, leading to impaired blood supply and subsequent tumor cell death. This effect is achieved by targeting the photosensitizers to the blood vessels and using a brief drug-light interval [23]. The vascular effects of PDT can be specifically directed to the tumor and its surrounding tissues, offering significant advantages over other PDT protocols that focus on photosensitizer accumulation within tumor cells themselves [27]. In addition to programmed apoptotic cell death, PDT also induces non-programmed necrotic cell death [28, 29], that results in the release of cellular components and molecules that provoke an inflammatory response [30]. PDT has been shown to induce several non-conventional cell death pathways in cancer cells, as well such as pyroptosis, necroptosis, ferroptosis, paraptosis and parthanatos [29]. In particular, the necrosis of tumor cells and vasculature induced by PDT can also activate CD8+ cytotoxic T lymphocytes, which target and destroy tumor cells while circulating in the body for extended periods [23, 28].
PTT operates independently of oxygen and utilizes NIR laser absorbers to generate heat, enabling thermal ablation of cancer cells under NIR laser exposure [15, 16]. Photothermal agents are administered intravenously or directly into the tumor, where they accumulate at the targeted site. When exposed to light at specific wavelengths, these agents absorb the light energy, causing them to shift from their ground state to an excited singlet state. The energy is then released through vibrational relaxation, a non-radiative decay process, in which the molecules return to their ground state by transferring energy to nearby molecules [31]. The elevation of kinetic energy during PTT leads to a rise in local tissue temperatures, thereby heating the surrounding microenvironment. When tissues reach 41°C, a heat-shock response is activated. This response leads to rapid changes in gene expression to counteract heat-induced damage, primarily through the production of heat-shock proteins [32]. At 42°C, tissue damage becomes irreversible. Prolonged exposure to temperatures between 42°C and 46°C for 10 minutes leads to substantial cell death. In the 46–52°C range, rapid cell death occurs due to microvascular thrombosis and subsequent ischemia. When tissue temperatures surpass 60°C, immediate cell death results from protein denaturation and the destruction of the plasma membrane [33]. However, research has demonstrated that temperatures surpassing 49 °C predominantly induce necrotic cell death, which may lead to inflammation and promote secondary tumor growth [34]. Notably, maintaining a highly controlled temperature range of 46–49 °C has been identified as optimal for eradicating tumors [35]. Within the NIR spectrum, the NIR-I window of 750–900 nm is currently the most widely used range in PTT research. However, there is growing interest in exploring the NIR-II range (wavelengths exceeding 1000 nm) to enhance therapeutic efficacy as the longer wavelengths of the NIR-II region reduce tissue scattering and have lower photon energy, enabling even greater tissue penetration depths [36]. Overall, phototherapies offers promising avenues in limiting tumor burden through innovative and targeted approaches.
Figure 1. Phototherapy in prostate cancer. Phototherapy represents a potential avenue for cancer treatment with promising options such as PDT and PTT. Under NIR light, PDT, with the help of photosensitizers, enhances immune response, devascularization and cell death based on induction of ROS, whereas PTT, with the help of photothermal agents, induces hyperthermia leading to heatshock response and cell death in prostate cancer cells.
Factors determining the efficacy of phototherapies in prostate cancer treatment
The application of phototherapies for treating prostate cancer involves a series of crucial steps. Initially, a photosensitizing or photothermal agent is introduced to the patient, either through systemic administration or direct injection into the tumor. The selection of the appropriate agent is influenced by various factors, including its ability to absorb light, distribute throughout the body, and preferentially accumulate in tumor cells [37, 38]. After the photosensitizing or photothermal agent has been adequately absorbed, a light source with specific characteristics, such as wavelength and power, is used to effectively activate the agent. The methods of light delivery can differ, with options such as intraluminal or interstitial illumination being employed [39]. For instance, in prostate cancer, intraluminal devices can be employed, where light-emitting instruments are introduced through catheters or endoscopes. Alternatively, interstitial phototherapy involves the direct placement of optical fibers or diffusers into prostate tissue, allowing light to penetrate deeper layers of the tumor [38, 39]. The ultimate goal is to achieve optimal light distribution throughout the tumor, ensuring maximum therapeutic effect. Employing active targeting strategies is also key to achieve focused therapeutic outcome along with minimal side-effects. Active targeting involves modifying nanoparticle delivery systems with surface coatings, such as antibodies, peptides, and aptamers, that specifically bind to molecules highly expressed on tumor surfaces or within the tumor microenvironment [40]. For instance, PSMA is predominantly found in castration-resistant, advanced, and metastatic prostate cancer, and has been identified as a key target [41]. For instance, PI-PEG on Au@PDA, creating Au@PDA/PEG-PI (target-NPS) nanoparticles have been designed for infrared-II laser-triggered phototheray. These nanoparticles effectively down-regulated PSMA expression in Prostate cancer cells. In vitro and in vivo experiments revealed strong photothermal conversion capabilities and photothermal stability while operating within the NIR range's maximum permissible exposure, highlighting their potential as photothermal agents [42]. In addition, a biocompatible melanin nanoparticles (PMNs-II-813) functionalized with a PSMA-specific small-molecule inhibitor has also been developed. This system enabled targeted prostate cancer treatment by combining radioisotope therapy with the phototherapy capabilities of PMNs-II-813, resulting in superior tumor inhibition rates compared to either radioisotope therapy and phototherapy alone [43]. These finding affirm that active targeting approaches exhibit improved performance and enhance the therapeutic efficacy of phototherapies against prostate cancer.
PDTs against prostate cancer
PDT holds great promise as a treatment modality for prostate cancer, potentially offering a safer and more effective alternative to traditional treatments [13, 44]. However, while PDT shows promise, it is unlikely to be fully effective in completely eliminating prostate cancer on its own. Therefore, combining PDT with other therapeutic approaches may enhance treatment outcomes by leveraging the strengths of each modality and compensating for their individual limitations, potentially resulting in synergistic or additive therapeutic effects [45]. In particular, combination strategies in PDT for the treatment of cancer aim to overcome challenges related to tumor size and location [46]. Larger tumors or those situated in difficult-to-reach areas present obstacles to complete tumor elimination with PDT alone, as light penetration is limited in depth [47]. Hence, integrating PDT with other therapeutic approaches, including surgery, chemotherapy, immunotherapy, and sonodynamic therapy can address these limitations (Figure 2) [48]. These combined approaches can enhance treatment efficacy, particularly for larger tumors, by sensitizing them or targeting remaining cancerous cells. Surgical intervention remains a common approach in the treatment of prostate cancer, though it does not always succeed in completely eradicating the disease. Recent research has explored the combination of surgery and PDT to improve treatment outcomes. For instance, a study has recently confirmed the feasibility, safety, and efficacy of combining surgery with PDT to treat locally recurrent prostate cancer while reporting superior short-term clinical outcomes [49]. Similarly, a retrospective analysis evaluated the safety and effectiveness of salvage radical prostatectomy performed after vascular-targeted PDT in 45 patients with persistent or recurrent disease. The findings indicated that this combined approach was both safe and effective for treating localized prostate cancer, with no severe complications or adverse effects reported [50]. Recently, scientists have introduced a new therapeutic strategy for prostate cancer called photochemotherapy, which integrates PDT with chemotherapy. This strategy allows for targeted drug delivery directly to tumor cells, potentially reducing damage to surrounding healthy tissues, unlike traditional chemotherapy [51]. The combination enhances treatment effectiveness, as chemotherapy compensates for PDT's limited light penetration and may increase the cancer cells' susceptibility to reactive oxygen species or hyperthermia, leading to a synergistic effect [52]. Additionally, a recent study has demonstrated that co-encapsulation of a theranostic photosensitizer, TPCI, and paclitaxel in liposomes results in up to a 30-fold increase in anticancer potency compared to standalone therapies. The treatment effectively ablated tumors and enabled precise, real-time monitoring of therapeutic responses in a mouse model with PC3 prostate tumors [53].
Photoimmunotherapy is an innovative treatment approach that integrates phototherapy and immunotherapy to combat cancer. This method aims to stimulate immune responses against tumors and prevent cancer recurrence [54]. This method selectively eradicates cancer cells by triggering the activating an immune response. NIR-photoimmunotherapy using the anti-prostate-specific membrane antigen (PSMA)-IR700 antibody demonstrated specific tumor targeting, significant tumor growth inhibition, and prolonged survival in a PSMA-expressing prostate cancer mouse model, with more than two-thirds of tumors cured. These findings suggest that anti-PSMA-IR700 is a promising therapeutic approach for PSMA-expressing tumors, with strong potential for clinical translation in humans [55]. Both PDT and sonodynamic therapy use sensitizers capable of producing reactive oxygen species that damage cancer cell membranes. Preclinical studies in other cancer types, such as brain cancer, have demonstrated positive outcomes from combining these two therapies [56]. While there are no direct studies investigating the combination of PDT and sonodynamic therapy for prostate cancer, ongoing research into their potential in cancer treatment is promising [57]. In the context of prostate cancer, ultrasound's deep penetration can activate photosensitizers without the need for an endoscope or light in the bladder, offering a unique advantage [56, 57]. Research is underway to identify the most effective sensitizers and delivery mechanisms to optimize the potential of PDT and its combination with other therapeutic modules in prostate cancer treatment. Overall, combining PDT with other conventional therapies is a promising avenue to reduce prostate cancer burden.
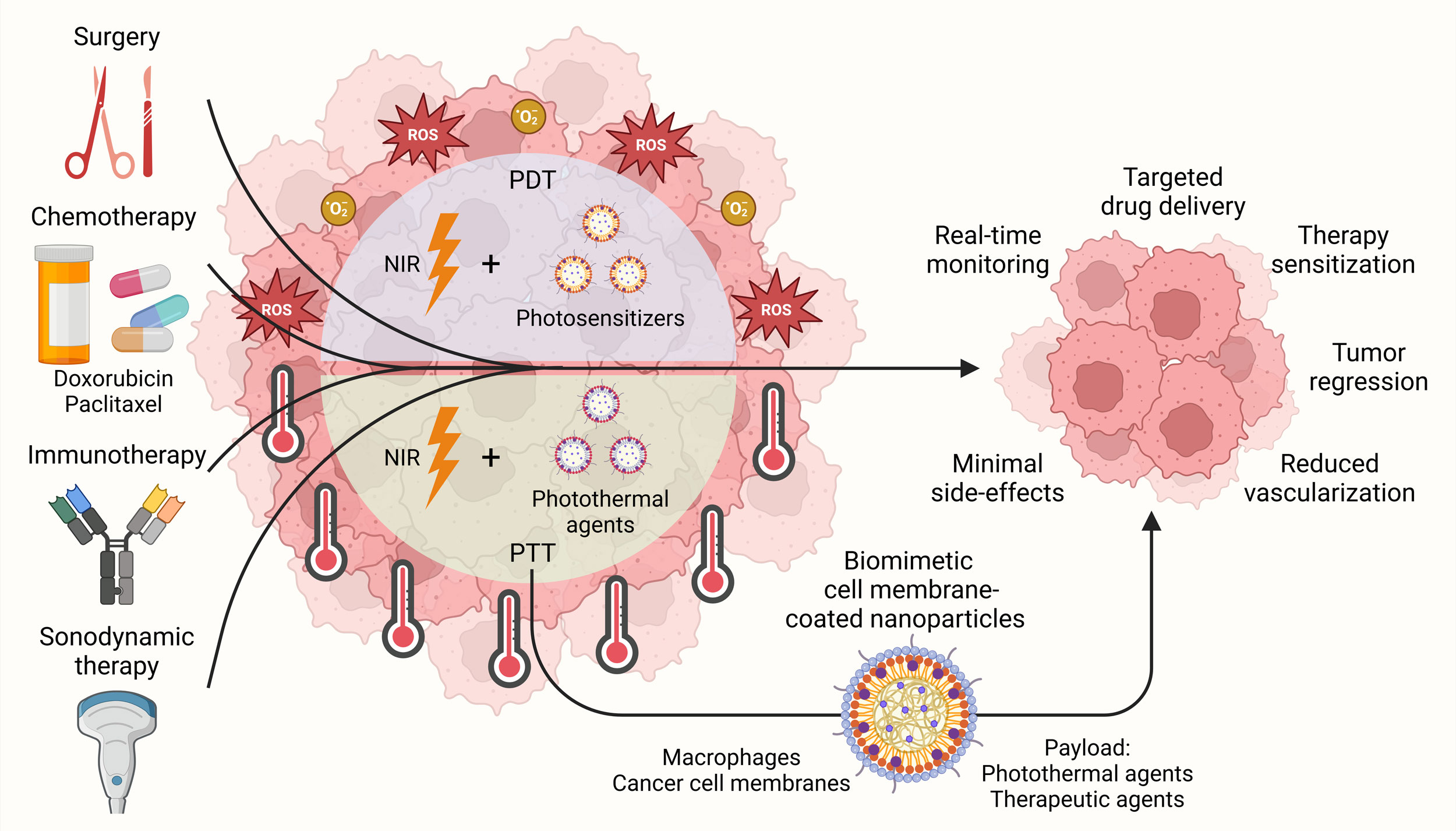 Figure 2. Combination therapeutic strategies involving phototherapies against prostate cancer. Therapeutic platforms combining phototherapies, such as PDT and PTT, with surgery, chemotherapy, immunotherapy and sonodynamic therapy have been devised for targeted drug delivery, improving therapy sensitization and inducing efficient tumor regression in prostate cancer while exhibiting minimal side-effects. In addition, biomimetic cell membrane-coated nanoparticles involving macrophages and cancer cell membrane have also been explored to enhance the delivery and efficacy of PTT.
Figure 2. Combination therapeutic strategies involving phototherapies against prostate cancer. Therapeutic platforms combining phototherapies, such as PDT and PTT, with surgery, chemotherapy, immunotherapy and sonodynamic therapy have been devised for targeted drug delivery, improving therapy sensitization and inducing efficient tumor regression in prostate cancer while exhibiting minimal side-effects. In addition, biomimetic cell membrane-coated nanoparticles involving macrophages and cancer cell membrane have also been explored to enhance the delivery and efficacy of PTT.
Photoimmunotherapy is an innovative treatment approach that integrates phototherapy and immunotherapy to combat cancer. This method aims to stimulate immune responses against tumors and prevent cancer recurrence [54]. This method selectively eradicates cancer cells by triggering the activating an immune response. NIR-photoimmunotherapy using the anti-prostate-specific membrane antigen (PSMA)-IR700 antibody demonstrated specific tumor targeting, significant tumor growth inhibition, and prolonged survival in a PSMA-expressing prostate cancer mouse model, with more than two-thirds of tumors cured. These findings suggest that anti-PSMA-IR700 is a promising therapeutic approach for PSMA-expressing tumors, with strong potential for clinical translation in humans [55]. Both PDT and sonodynamic therapy use sensitizers capable of producing reactive oxygen species that damage cancer cell membranes. Preclinical studies in other cancer types, such as brain cancer, have demonstrated positive outcomes from combining these two therapies [56]. While there are no direct studies investigating the combination of PDT and sonodynamic therapy for prostate cancer, ongoing research into their potential in cancer treatment is promising [57]. In the context of prostate cancer, ultrasound's deep penetration can activate photosensitizers without the need for an endoscope or light in the bladder, offering a unique advantage [56, 57]. Research is underway to identify the most effective sensitizers and delivery mechanisms to optimize the potential of PDT and its combination with other therapeutic modules in prostate cancer treatment. Overall, combining PDT with other conventional therapies is a promising avenue to reduce prostate cancer burden.
Figure 2. Combination therapeutic strategies involving phototherapies against prostate cancer. Therapeutic platforms combining phototherapies, such as PDT and PTT, with surgery, chemotherapy, immunotherapy and sonodynamic therapy have been devised for targeted drug delivery, improving therapy sensitization and inducing efficient tumor regression in prostate cancer while exhibiting minimal side-effects. In addition, biomimetic cell membrane-coated nanoparticles involving macrophages and cancer cell membrane have also been explored to enhance the delivery and efficacy of PTT.
PTTs against prostate cancer
PTT offers significant clinical promise due to its advantages of high efficiency, minimal invasiveness, and remarkable selectivity [14]. In addition to enhancing the targeting capabilities of photothermal agents, improving their inherent properties such as enhancing photothermal conversion efficiency, photostability, and other physical attributes, while simultaneously improving biocompatibility and minimizing cytotoxic effects have substantially improved the worth of PTT as therapeutic modality [58]. For instance, a microemulsion approach was employed to develop IR780-MnCs, which integrate poly(lactic-co-glycolic acid) (PLGA), magnetic Fe₃O₄ nanoparticles, and IR780 dye to enhance photothermal therapy for prostate tumors. These biocompatible nanoparticles exhibited stable performance, controlled release in acidic environments, extended circulation times, and effective tumor targeting due to their optimal size and enhanced permeability and retention effect. Under 808 nm laser irradiation, the heat generated by IR780 enabled efficient PTT. Both in vitro and in vivo experiments demonstrated that IR780-MnCs achieved significantly stronger anti-tumor effects against prostate cancer compared to control groups [59]. In another study, AuNC@SiO₂ nanoparticles with a size of 60–70 nm, have been characterized by low cytotoxicity and improved photostability. These nanoparticles were evaluated as NIR photothermal agents for treating prostate cancer both in vitro and in vivo. During NIR irradiation at an 808 nm wavelength, the PTT experiment demonstrated effective tumor ablation in PC-3 cancer cells. In vivo studies further revealed a progressive reduction in tumor volume in tumor-bearing mice over 15 days of NIR irradiation, culminating in complete tumor disappearance [60]. Furthermore, a simple and rapid two-minute microwave-assisted method for synthesizing atomically thin copper nanocrystals has been introduced. To enhance their biocompatibility, aqueous stability, water dispersibility, and free carrier density, these nanocrystals were coated with starch layers. In vitro experiments on human prostate cancer PC-3/Luc+ cells demonstrated a high photothermal ablation effect, with an impressive 98.4% of the cells being eradicated [61]. A nanosystem (AuNCs–LHRHa) that integrates fluorescence/computed tomography (FL/CT) imaging and PTT through 808 nm NIR irradiation has also been devised. Functionalized with LHRHa, the nanoparticles achieved enhanced tumor targeting by exploiting GnRHR overexpression in prostate cancer cells, resulting in improved therapeutic outcomes compared to non-targeted groups [62]. In addition, AMNDs-LHRH nanosystems incorporating Au/Mn nanodots for treating bone metastatic Prostate cancer have been devised. These systems exhibited excellent targeting capabilities and photothermal response, as demonstrated in a mouse tibial prostate cancer model, where the tumor site rapidly reached 50 °C under 808 nm laser irradiation [63]. These finding affirm beneficial impacts of PTT as prostate cancer treatment.
The potential of combining PTT with other therapeutic strategies for prostate cancer has garnered substantial attention in recent years as combination treatment modalities enhance overall therapeutic outcomes (Figure 2) [64]. Recent studies have explored various synergistic approaches. For instance, PSMA-targeted light-responsive nanosystems combining PTT and chemotherapy have been devised. These systems were designed with liquid perfluorocarbon cores and polymer shells, incorporating IR780 (an indocyanine green derivative) along with the chemotherapeutic agent paclitaxel.The perfluorocarbon component facilitated ultrasound-enhanced drug delivery and release via a gas–liquid transition, while IR780 enabled photoacoustic imaging-guided PTT. The combined therapy demonstrated excellent inhibitory effects on tumor cell proliferation in vitro and significant therapeutic efficacy in vivo [65]. In another approach, a Cu-MNCS-AIPH@PAA nanoplatform with excellent photothermal conversion and fenton-like reaction efficiency, have been developed. This platform synergistically combines PTT, chemodynamic therapy, and alkyl radical production, effectively inhibiting tumor growth in vitro and in vivo [66]. Similarly, SPION-based Eto delivery systems combined with mild hyperthermia (808 nm laser irradiation) to target androgen-dependent and independent prostate cancer cells. Their Eto-BSA@PAA@SPIONs showed increased drug release and cell sensitization to chemotherapy, significantly improving cytotoxicity and inducing ~50% more Eto release in nanoparticles [67]. A multifunctional nanoparticle system based on mesoporous polydopamine for targeted drug delivery and chemo-PTT of prostate cancer have been explored. The nanoparticles, AS1411@MPDA-DTX, were functionalized with the aptamer AS1411, which specifically binds to surface nucleolin expressed on prostate cancer cells. The system demonstrated effective tumor targeting, pH-responsive drug release, and enhanced anti-cancer efficacy under NIR irradiation in vitro and in vivo [68]. Additionally, doxorubicin-supported reduced graphene oxide (RGO-HNP) nanoparticles have been introduced which are stabilized by chitosan. This system achieved controlled doxorubicin release (~50% over 48 hours), high biocompatibility, and efficient heat conversion under 808 nm irradiation, demonstrating significant tumor cell death [69]. Furthermore, PLGA-ICG-R848 nanoparticles co-loaded with indocyanine green and TLR7/8 agonist R848 have been developed. Under NIR laser irradiation, this system inhibited prostate cancer cell growth and enhanced anti-tumor immunity in a mouse model, as evidenced by increased dendritic cell maturation [70]. Moreover, another platform named GCR-CDP8MA for IR-II-mediated photothermal immunotherapy has also been devised. Functionalized with gamma-Cd cross-linked polyethylenimine, targeting peptides, and meclofenamic acid, this system exhibited remarkable biocompatibility and efficient photothermal conversion when exposed to 1208 nm laser irradiation. It enhanced m6A RNA methylation, reducing PD-L1 transcript stability and promoting immune clearance through T-cell activation and maturation of dendritic cells [71]. Overall, combining PTT with other conventional therapies is a promising avenue to reduce prostate cancer burden.
The potential of combining PTT with other therapeutic strategies for prostate cancer has garnered substantial attention in recent years as combination treatment modalities enhance overall therapeutic outcomes (Figure 2) [64]. Recent studies have explored various synergistic approaches. For instance, PSMA-targeted light-responsive nanosystems combining PTT and chemotherapy have been devised. These systems were designed with liquid perfluorocarbon cores and polymer shells, incorporating IR780 (an indocyanine green derivative) along with the chemotherapeutic agent paclitaxel.The perfluorocarbon component facilitated ultrasound-enhanced drug delivery and release via a gas–liquid transition, while IR780 enabled photoacoustic imaging-guided PTT. The combined therapy demonstrated excellent inhibitory effects on tumor cell proliferation in vitro and significant therapeutic efficacy in vivo [65]. In another approach, a Cu-MNCS-AIPH@PAA nanoplatform with excellent photothermal conversion and fenton-like reaction efficiency, have been developed. This platform synergistically combines PTT, chemodynamic therapy, and alkyl radical production, effectively inhibiting tumor growth in vitro and in vivo [66]. Similarly, SPION-based Eto delivery systems combined with mild hyperthermia (808 nm laser irradiation) to target androgen-dependent and independent prostate cancer cells. Their Eto-BSA@PAA@SPIONs showed increased drug release and cell sensitization to chemotherapy, significantly improving cytotoxicity and inducing ~50% more Eto release in nanoparticles [67]. A multifunctional nanoparticle system based on mesoporous polydopamine for targeted drug delivery and chemo-PTT of prostate cancer have been explored. The nanoparticles, AS1411@MPDA-DTX, were functionalized with the aptamer AS1411, which specifically binds to surface nucleolin expressed on prostate cancer cells. The system demonstrated effective tumor targeting, pH-responsive drug release, and enhanced anti-cancer efficacy under NIR irradiation in vitro and in vivo [68]. Additionally, doxorubicin-supported reduced graphene oxide (RGO-HNP) nanoparticles have been introduced which are stabilized by chitosan. This system achieved controlled doxorubicin release (~50% over 48 hours), high biocompatibility, and efficient heat conversion under 808 nm irradiation, demonstrating significant tumor cell death [69]. Furthermore, PLGA-ICG-R848 nanoparticles co-loaded with indocyanine green and TLR7/8 agonist R848 have been developed. Under NIR laser irradiation, this system inhibited prostate cancer cell growth and enhanced anti-tumor immunity in a mouse model, as evidenced by increased dendritic cell maturation [70]. Moreover, another platform named GCR-CDP8MA for IR-II-mediated photothermal immunotherapy has also been devised. Functionalized with gamma-Cd cross-linked polyethylenimine, targeting peptides, and meclofenamic acid, this system exhibited remarkable biocompatibility and efficient photothermal conversion when exposed to 1208 nm laser irradiation. It enhanced m6A RNA methylation, reducing PD-L1 transcript stability and promoting immune clearance through T-cell activation and maturation of dendritic cells [71]. Overall, combining PTT with other conventional therapies is a promising avenue to reduce prostate cancer burden.
Biomimetic cell membrane-coated nanoparticles have also been employed for active targeting (Figure 2). For instance, a nano-platform by encapsulating autophagy inhibitors and chloroquine within mesoporous polydopamine nanoparticles coated with homologous prostate cancer cell membranes have been developed. This biomimetic system synergistically combined PTT and autophagy inhibition, effectively suppressing tumor growth in vitro and in vivo [72]. A novel macrophage-based drug delivery system (MAs-DOX/rGO) has also been explored. Graphene oxide loaded with doxorubicin (DOX/rGO) was internalized into macrophages, leveraging their natural chemotaxis to deliver the system to tumors. Upon NIR irradiation, the heat generated by DOX/rGO caused macrophage destruction, releasing doxorubicin into the tumor microenvironment. In vitro and in vivo studies confirmed the synergistic efficacy of this chemotherapy-PTT combination for Prostate cancer [73]. In addition, biomimetic Fe₂O₃ nanoclusters modified with polypyrrole and cell membranes. These nanoclusters exhibited exceptional absorption in the NIR-II window and a photothermal conversion efficiency of 78.7% under 1064 nm irradiation, enabling low-dose PTT with excellent biocompatibility [74]. Overall, these findings highlight the biomimetic applications of PTT and their beneficial impact against prostate cancer.
Combining PDT and PTT as prostate cancer therapy
In addition to combining PDT and PTT independently with conventional therapies, the combination of PDT and PTT has also been explored to enhance the benefits of both therapies. Thermal effect by PTT can improve local blood circulation and increase oxygen levels within the tumor, thereby compensating for the hypoxic conditions that limit PDT's effectiveness [75]. For instance, self-assembled nanoparticles, like polydopamine nanoparticles, have been utilized to co-deliver photodynamic and photothermal agents, achieving a synergistic therapeutic outcome [45, 75]. In addition, graphene oxide modified with palladium nanoparticles (GO-Pd NPs) for combined PDT and PTT have also been developed. Under NIR laser irradiation, GO-Pd NPs generated high photothermal and reactive oxygen species effects, leading to reduced tumor volumes in prostate cancer models with minimal toxicity to healthy organs. This combination therapy showed strong potential for localized solid tumor treatment [76]. Furthermore, gold-caged copolymer nanoparticles (PTX-PP@Au NPs) have recently been developed as a multifunctional platform for androgen-resistant prostate cancer. These nanoparticles encapsulated paclitaxel within gold-caged pluronic-polyethylenimine micelles. Single-light activation (808 nm) enabled synergistic PTT and PDT effects while enhancing release through photothermal activation. In vitro, the system demonstrated enhanced cell uptake, cell cycle arrest, apoptosis, and TRPV6 ion channel blockage, whereas in vivo, PTX-PP@Au NPs achieved high tumor accumulation via enhanced permeability and retention effects, supporting their use as a robust multimodal therapy [77]. Moreover, a multifunctional nanoplatform GNS@IR820/DTX-CD133 has demonstrated effective targeting of tumor tissues in CRPC through CD133 antibody guidance and enabled real-time monitoring via NIR fluorescence and photoacoustic imaging. The synergistic PDT, PTT and chemotherapy strategies under NIR-light irradiation have been shown to achieve excellent antitumor effects in vitro and in vivo, highlighting its potential for clinical applications in CRPC therapy [78]. Finally, polymeric vesicles functionalized with AuNR surfaces achieved synergistic PDT and PTT under single-wavelength NIR excitation, demonstrating high cellular uptake, efficient tumor accumulation, and enhanced photothermal conversion, significantly promoting apoptosis in androgen-independent PC3 prostate cancer cells [79]. These findings highlight the potential of combining PDT and PTT as potent therapeutic option against prostate cancer.
Conclusion and future prospects
Prostate cancer is one of the primary causes of cancer-related fatalities among men, and the majority of patients undergoing androgen deprivation therapy eventually develop mCRPC, highlighting the challenges of standard treatment approaches. Phototherapies, particularly PDT and PTT, represent a promising frontier in prostate cancer management, offering innovative solutions to challenges associated with traditional treatments. PDT harnesses the production of reactive oxygen species to selectively destroy cancer cells while inducing anti-tumor immune responses. Complementarily, PTT employs localized hyperthermia to ablate tumors with minimal off-target effects. These therapies benefit from the use of NIR light, which achieves deeper tissue penetration and reduced collateral damage compared to other wavelengths. Recent advancements in nanoparticle design and functionalization have enhanced the targeting efficiency and therapeutic outcomes of PDT and PTT against prostate cancer. For example, nanoparticles functionalized with PSMA-specific ligands enable precise delivery to prostate cancer cells, improving treatment specificity. Combination strategies, such as integrating PDT and PTT with chemotherapy or immunotherapy, have demonstrated synergistic effects.
Despite advances in understanding the mechanisms behind phototherapies and creating innovative nanomaterials, challenges such as lack of highly efficient photosensitizers and photothermal agents, optimizing light delivery, minimizing systemic toxicity, and scaling production for clinical use remain [38]. Multimodal therapies combining PDT with other treatments have shown potential in addressing issues related to multidrug-resistant and hypoxia-induced prostate cancers [80]. However, these strategies introduce complexities, such as increased side effects and the need for careful optimization of sequencing and timing. There has been a global effort to develop novel organic photosensitizers to improve the efficiency of PDT [81]. In recent advancements, PDT has entered a new phase involving vectorization and encapsulation techniques within drug delivery systems. These innovative strategies are aimed at improving the targeting and delivery of photosensitizers directly to tumor tissues [82-84]. Over the past five years, clinical research on the use of PTT for prostate cancer has been limited, with many studies focusing on the application of gold nanoparticles as the primary photothermal agents [85]. The limited number of clinical studies stems mainly from difficulties associated with the prostate's deep anatomical location and the prolonged process of advancing photothermal agents from basic research to clinical trials. Additionally, a significant drawback of PTT for solid tumor treatment is the inadequate penetration of light, which may prevent complete tumor eradication and increase the risk of metastasis or recurrence [86]. In addition, full potential of combining PDT and PTT is also challenged by challenges remain with the low photoconversion efficiency of some materials [87], warranting considerable improvement to enhance the efficacy of these phototherpies against prostate cancer. Lastly, further clinical studies are essential to explore the effectiveness of phototherapies, both as a standalone treatment and in combination with other cancer therapies [13]. As these therapies continue to evolve, they hold the potential to significantly improve outcomes for patients with prostate cancer, particularly those with advanced or treatment-resistant forms of the disease. By integrating phototherapies into standard care protocols, the global burden of prostate cancer could be markedly reduced, paving the way for more personalized and effective treatment strategies.
Despite advances in understanding the mechanisms behind phototherapies and creating innovative nanomaterials, challenges such as lack of highly efficient photosensitizers and photothermal agents, optimizing light delivery, minimizing systemic toxicity, and scaling production for clinical use remain [38]. Multimodal therapies combining PDT with other treatments have shown potential in addressing issues related to multidrug-resistant and hypoxia-induced prostate cancers [80]. However, these strategies introduce complexities, such as increased side effects and the need for careful optimization of sequencing and timing. There has been a global effort to develop novel organic photosensitizers to improve the efficiency of PDT [81]. In recent advancements, PDT has entered a new phase involving vectorization and encapsulation techniques within drug delivery systems. These innovative strategies are aimed at improving the targeting and delivery of photosensitizers directly to tumor tissues [82-84]. Over the past five years, clinical research on the use of PTT for prostate cancer has been limited, with many studies focusing on the application of gold nanoparticles as the primary photothermal agents [85]. The limited number of clinical studies stems mainly from difficulties associated with the prostate's deep anatomical location and the prolonged process of advancing photothermal agents from basic research to clinical trials. Additionally, a significant drawback of PTT for solid tumor treatment is the inadequate penetration of light, which may prevent complete tumor eradication and increase the risk of metastasis or recurrence [86]. In addition, full potential of combining PDT and PTT is also challenged by challenges remain with the low photoconversion efficiency of some materials [87], warranting considerable improvement to enhance the efficacy of these phototherpies against prostate cancer. Lastly, further clinical studies are essential to explore the effectiveness of phototherapies, both as a standalone treatment and in combination with other cancer therapies [13]. As these therapies continue to evolve, they hold the potential to significantly improve outcomes for patients with prostate cancer, particularly those with advanced or treatment-resistant forms of the disease. By integrating phototherapies into standard care protocols, the global burden of prostate cancer could be markedly reduced, paving the way for more personalized and effective treatment strategies.
Declaration
Acknowledgements
None.
Ethical policy
Non applicable.
Availability of data and materials
All data generated or analysed during this study are included in this publication.
Author contributions
AU searched academic literature, wrote the draft manuscript, drew the figures and submitted the final manuscript online.
Competing interests
None.
Funding
None.
None.
Ethical policy
Non applicable.
Availability of data and materials
All data generated or analysed during this study are included in this publication.
Author contributions
AU searched academic literature, wrote the draft manuscript, drew the figures and submitted the final manuscript online.
Competing interests
None.
Funding
None.
References
- Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, Jemal A: Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2024, 74(3): 229-263.
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F: Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021, 71(3): 209-249.
- Foreman KJ, Marquez N, Dolgert A, Fukutaki K, Fullman N, McGaughey M, Pletcher MA, Smith AE, Tang K, Yuan CW, et al: Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet 2018, 392(10159): 2052-2090.
- Wang K, Ruan H, Xu T, Liu L, Liu D, Yang H, Zhang X, Chen K: Recent advances on the progressive mechanism and therapy in castration-resistant prostate cancer. Onco Targets Ther 2018, 11: 3167-3178.
- Qi Z, Xu Z, Zhang L, Zou Y, Li J, Yan W, Li C, Liu N, Wu H: Overcoming resistance to immune checkpoint therapy in PTEN-null prostate cancer by intermittent anti-PI3Kα/β/δ treatment. Nat Commun 2022, 13(1): 182.
- Wilkinson S, Ye H, Karzai F, Harmon SA, Terrigino NT, VanderWeele DJ, Bright JR, Atway R, Trostel SY, Carrabba NV, et al: Nascent Prostate Cancer Heterogeneity Drives Evolution and Resistance to Intense Hormonal Therapy. Eur Urol 2021, 80(6): 746-757.
- Wang K, Ma F, Arai S, Wang Y, Varkaris A, Poluben L, Voznesensky O, Xie F, Zhang X, Yuan X, et al: WNT5a Signaling through ROR2 Activates the Hippo Pathway to Suppress YAP1 Activity and Tumor Growth. Cancer Res 2023, 83(7): 1016-1030.
- Kishan AU, Sun Y, Hartman H, Pisansky TM, Bolla M, Neven A, Steigler A, Denham JW, Feng FY, Zapatero A, et al: Androgen deprivation therapy use and duration with definitive radiotherapy for localised prostate cancer: an individual patient data meta-analysis. Lancet Oncol 2022, 23(2): 304-316.
- Lestingi JFP, Guglielmetti GB, Trinh QD, Coelho RF, Pontes J, Jr., Bastos DA, Cordeiro MD, Sarkis AS, Faraj SF, Mitre AI, et al: Extended Versus Limited Pelvic Lymph Node Dissection During Radical Prostatectomy for Intermediate- and High-risk Prostate Cancer: Early Oncological Outcomes from a Randomized Phase 3 Trial. Eur Urol 2021, 79(5): 595-604.
- Rebello RJ, Oing C, Knudsen KE, Loeb S, Johnson DC, Reiter RE, Gillessen S, Van der Kwast T, Bristow RG: Prostate cancer. Nat Rev Dis Primers 2021, 7(1): 9.
- Kulasegaran T, Oliveira N: Metastatic Castration-Resistant Prostate Cancer: Advances in Treatment and Symptom Management. Curr Treat Options Oncol 2024, 25(7): 914-931.
- Le TK, Duong QH, Baylot V, Fargette C, Baboudjian M, Colleaux L, Taïeb D, Rocchi P: Castration-Resistant Prostate Cancer: From Uncovered Resistance Mechanisms to Current Treatments. Cancers (Basel) 2023, 15(20): 5047.
- Wahnou H, Youlyouz-Marfak I, Liagre B, Sol V, Oudghiri M, Duval RE, Limami Y: Shining a Light on Prostate Cancer: Photodynamic Therapy and Combination Approaches. Pharmaceutics 2023, 15(6): 1767.
- Dong Z, Xue K, Verma A, Shi J, Wei Z, Xia X, Wang K, Zhang X: Photothermal therapy: a novel potential treatment for prostate cancer. Biomater Sci 2024, 12(10): 2480-2503.
- Fang L, Chen Z, Dai J, Pan Y, Tu Y, Meng Q, Diao Y, Yang S, Guo W, Li L, et al: Recent Advances in Strategies to Enhance Photodynamic and Photothermal Therapy Performance of Single-Component Organic Phototherapeutic Agents. Adv Sci (Weinh) 2025, Epub ahead of print: e2409157.
- Hemmer E, Venkatachalam N, Hyodo H, Hattori A, Ebina Y, Kishimoto H, Soga K: Upconverting and NIR emitting rare earth based nanostructures for NIR-bioimaging. Nanoscale 2013, 5(23): 11339-11361.
- Vogel A, Venugopalan V: Mechanisms of pulsed laser ablation of biological tissues. Chem Rev 2003, 103(2): 577-644.
- Weissleder R: A clearer vision for in vivo imaging. Nat Biotechnol 2001, 19(4): 316-317.
- Jacques SL: Optical properties of biological tissues: a review. Phys Med Biol 2013, 58(11): R37-61.
- Stolik S, Delgado JA, Pérez A, Anasagasti L: Measurement of the penetration depths of red and near infrared light in human "ex vivo" tissues. J Photochem Photobiol B 2000, 57(2-3): 90-93.
- Tsai MF, Chang SH, Cheng FY, Shanmugam V, Cheng YS, Su CH, Yeh CS: Au nanorod design as light-absorber in the first and second biological near-infrared windows for in vivo photothermal therapy. ACS Nano 2013, 7(6): 5330-5342.
- Beşbınar Ö B, Uyar R, Yilmazer A: Omic Evaluation of Nanomaterial-Based Photodynamic Therapy of Cancer. Methods Mol Biol 2024, 2835: 277-288.
- Kwiatkowski S, Knap B, Przystupski D, Saczko J, Kędzierska E, Knap-Czop K, Kotlińska J, Michel O, Kotowski K, Kulbacka J: Photodynamic therapy - mechanisms, photosensitizers and combinations. Biomed Pharmacother 2018, 106: 1098-1107.
- Correia JH, Rodrigues JA, Pimenta S, Dong T, Yang Z: Photodynamic Therapy Review: Principles, Photosensitizers, Applications, and Future Directions. Pharmaceutics 2021, 13(9): 1332.
- Mohan R, Schellhammer PF: Treatment options for localized prostate cancer. Am Fam Physician 2011, 84(4): 413-420.
- Rodrigues MC, de Sousa Júnior WT, Mundim T, Vale CLC, de Oliveira JV, Ganassin R, Pacheco TJA, Vasconcelos Morais JA, Longo JPF, Azevedo RB, et al: Induction of Immunogenic Cell Death by Photodynamic Therapy Mediated by Aluminum-Phthalocyanine in Nanoemulsion. Pharmaceutics 2022, 14(1): 196.
- Plekhova N, Shevchenko O, Korshunova O, Stepanyugina A, Tananaev I, Apanasevich V: Development of Novel Tetrapyrrole Structure Photosensitizers for Cancer Photodynamic Therapy. Bioengineering (Basel) 2022, 9(2): 82.
- Tan L, Shen X, He Z, Lu Y: The Role of Photodynamic Therapy in Triggering Cell Death and Facilitating Antitumor Immunology. Front Oncol 2022, 12: 863107.
- Mishchenko T, Balalaeva I, Gorokhova A, Vedunova M, Krysko DV: Which cell death modality wins the contest for photodynamic therapy of cancer? Cell Death Dis 2022, 13(5): 455.
- Hamblin MR: Photodynamic Therapy for Cancer: What's Past is Prologue. Photochem Photobiol 2020, 96(3): 506-516.
- Li C, Cheng Y, Li D, An Q, Zhang W, Zhang Y, Fu Y: Antitumor Applications of Photothermal Agents and Photothermal Synergistic Therapies. Int J Mol Sci 2022, 23(14): 7909.
- Richter K, Haslbeck M, Buchner J: The heat shock response: life on the verge of death. Mol Cell 2010, 40(2): 253-266.
- Knavel EM, Brace CL: Tumor ablation: common modalities and general practices. Tech Vasc Interv Radiol 2013, 16(4): 192-200.
- Golstein P, Kroemer G: Cell death by necrosis: towards a molecular definition. Trends Biochem Sci 2007, 32(1): 37-43.
- Christofferson DE, Yuan J: Necroptosis as an alternative form of programmed cell death. Curr Opin Cell Biol 2010, 22(2): 263-268.
- Upputuri PK, Pramanik M: Photoacoustic imaging in the second near-infrared window: a review. J Biomed Opt 2019, 24(4): 1-20.
- van Straten D, Mashayekhi V, de Bruijn HS, Oliveira S, Robinson DJ: Oncologic Photodynamic Therapy: Basic Principles, Current Clinical Status and Future Directions. Cancers (Basel) 2017, 9(2): 19.
- Zhang Y, Zhang Y, Zhang G, Wu J, Wang L, Dong Z, Zheng Y, Huang Q, Zou M, Liao R: Recent advances and clinical challenges of phototherapeutic nanoparticles in cancer monotherapy or combination therapy. Coord Chem Rev 2024, 518: 216069.
- Moore CM, Pendse D, Emberton M: Photodynamic therapy for prostate cancer--a review of current status and future promise. Nat Clin Pract Urol 2009, 6(1): 18-30.
- Li J, Wang Q, Xia G, Adilijiang N, Li Y, Hou Z, Fan Z, Li J: Recent Advances in Targeted Drug Delivery Strategy for Enhancing Oncotherapy. Pharmaceutics 2023, 15(9): 2233.
- Wang F, Li Z, Feng X, Yang D, Lin M: Advances in PSMA-targeted therapy for prostate cancer. Prostate Cancer Prostatic Dis 2022, 25(1): 11-26.
- Ding X, Bai S, Liu F, Michał N, Roman S, Peng N, Liu Y: NIR-II-triggered photothermal therapy with Au@PDA/PEG-PI for targeted downregulation of PSMA in prostate cancer. Acta Biomater 2023, 157: 487-499.
- Xia L, Meng X, Wen L, Zhou N, Liu T, Xu X, Wang F, Cheng Z, Yang Z, Zhu H: A Highly Specific Multiple Enhancement Theranostic Nanoprobe for PET/MRI/PAI Image-Guided Radioisotope Combined Photothermal Therapy in Prostate Cancer. Small 2021, 17(21): e2100378.
- Algorri JF, Ochoa M, Roldán-Varona P, Rodríguez-Cobo L, López-Higuera JM: Photodynamic Therapy: A Compendium of Latest Reviews. Cancers (Basel) 2021, 13(17): 4447.
- Xue Q, Zhang J, Jiao J, Qin W, Yang X: Photodynamic therapy for prostate cancer: Recent advances, challenges and opportunities. Front Oncol 2022, 12: 980239.
- Ito Y, Udo K, Vertosick EA, Sjoberg DD, Vickers AJ, Al-Ahmadie HA, Chen YB, Gopalan A, Sirintrapun SJ, Tickoo SK, et al: Clinical Usefulness of Prostate and Tumor Volume Related Parameters following Radical Prostatectomy for Localized Prostate Cancer. J Urol 2019, 201(3): 535-540.
- Osuchowski M, Aebisher D, Bartusik-Aebisher D, Krupka-Olek M, Dynarowicz K, Przygoda M, Kawczyk-Krupka A: Photodynamic Therapy-Adjunctive Therapy in the Treatment of Prostate Cancer. Diagnostics (Basel) 2022, 12(5): 1113.
- Borgia F, Giuffrida R, Caradonna E, Vaccaro M, Guarneri F, Cannavò SP: Early and Late Onset Side Effects of Photodynamic Therapy. Biomedicines 2018, 6(1): 12.
- Lebdai S, Villers A, Barret E, Nedelcu C, Bigot P, Azzouzi AR: Feasibility, safety, and efficacy of salvage radical prostatectomy after Tookad® Soluble focal treatment for localized prostate cancer. World J Urol 2015, 33(7): 965-971.
- Pierrard V, Lebdai S, Kleinclauss F, Azzouzi AR, Terrier JE, Fortier E, Joniau S, Van Der Poel H, Salomon G, Casanova J, et al: Radical Prostatectomy after Vascular Targeted Photodynamic Therapy with Padeliporfin: Feasibility, and Early and Intermediate Results. J Urol 2019, 201(2): 315-321.
- Li G, Wang C, Jin B, Sun T, Sun K, Wang S, Fan Z: Advances in smart nanotechnology-supported photodynamic therapy for cancer. Cell Death Discov 2024, 10(1): 466.
- Poudel BK, Soe ZC, Ruttala HB, Gupta B, Ramasamy T, Thapa RK, Gautam M, Ou W, Nguyen HT, Jeong JH, et al: In situ fabrication of mesoporous silica-coated silver-gold hollow nanoshell for remotely controllable chemo-photothermal therapy via phase-change molecule as gatekeepers. Int J Pharm 2018, 548(1): 92-103.
- Wang X, Tong J, He Z, Yang X, Meng F, Liang H, Zhang X, Luo L: Paclitaxel-Potentiated Photodynamic Theranostics for Synergistic Tumor Ablation and Precise Anticancer Efficacy Monitoring. ACS Appl Mater Interfaces 2020, 12(5): 5476-5487.
- Mohiuddin TM, Zhang C, Sheng W, Al-Rawe M, Zeppernick F, Meinhold-Heerlein I, Hussain AF: Near Infrared Photoimmunotherapy: A Review of Recent Progress and Their Target Molecules for Cancer Therapy. Int J Mol Sci 2023, 24(3): 2655.
- Nagaya T, Nakamura Y, Okuyama S, Ogata F, Maruoka Y, Choyke PL, Kobayashi H: Near-Infrared Photoimmunotherapy Targeting Prostate Cancer with Prostate-Specific Membrane Antigen (PSMA) Antibody. Mol Cancer Res 2017, 15(9): 1153-1162.
- Borah BM, Cacaccio J, Durrani FA, Bshara W, Turowski SG, Spernyak JA, Pandey RK: Sonodynamic therapy in combination with photodynamic therapy shows enhanced long-term cure of brain tumor. Sci Rep 2020, 10(1): 21791.
- Hu X, Zhang YS, Liu YC, Wang N, Zeng XT, Zhang LL: Emerging photodynamic/sonodynamic therapies for urological cancers: progress and challenges. J Nanobiotechnology 2022, 20(1): 437.
- Du B, Ma C, Ding G, Han X, Li D, Wang E, Wang J: Cooperative Strategies for Enhancing Performance of Photothermal Therapy (PTT) Agent: Optimizing Its Photothermal Conversion and Cell Internalization Ability. Small 2017, 13(13): 1603275.
- Li S, Ma Y, Ma C, Shi L, Li F, Chang L: NIR-triggerable self-assembly multifunctional nanocarriers to enhance the tumor penetration and photothermal therapy efficiency for castration-resistant prostate cancer. Discov Nano 2023, 18(1): 46.
- Kim J, Chun SH, Amornkitbamrung L, Song C, Yuk JS, Ahn SY, Kim BW, Lim YT, Oh BK, Um SH: Gold nanoparticle clusters for the investigation of therapeutic efficiency against prostate cancer under near-infrared irradiation. Nano Converg 2020, 7(1): 5.
- Zheng Z, Yu P, Cao H, Cheng M, Zhou T, Lee LE, Ulstrup J, Zhang J, Engelbrekt C, Ma L: Starch Capped Atomically Thin CuS Nanocrystals for Efficient Photothermal Therapy. Small 2021, 17(47): e2103461.
- Wang Z, He L, Che S, Xing H, Guan L, Yang Z, Li X, Zvyagin AV, Lin Q, Qu W: AuNCs-LHRHa nano-system for FL/CT dual-mode imaging and photothermal therapy of targeted prostate cancer. J Mater Chem B 2022, 10(27): 5182-5190.
- Wang Z, Xing H, Liu A, Guan L, Li X, He L, Sun Y, Zvyagin AV, Yang B, Lin Q: Multifunctional nano-system for multi-mode targeted imaging and enhanced photothermal therapy of metastatic prostate cancer. Acta Biomater 2023, 166: 581-592.
- Ferroni C, Del Rio A, Martini C, Manoni E, Varchi G: Light-Induced Therapies for Prostate Cancer Treatment. Front Chem 2019, 7: 719.
- Xiao L, Wu Y, Dai J, Zhang W, Cao Y: Laser-activated nanoparticles for ultrasound/photoacoustic imaging-guided prostate cancer treatment. Front Bioeng Biotechnol 2023, 11: 1141984.
- Xu B, Niu R, Tang Y, Wang C, Jin L, Wang Y: A Cu-based nanoplatform for near-infrared light amplified multi-mode prostate cancer specific therapy. J Mater Chem B 2022, 10(37): 7628-7633.
- Onbasli K, Erkısa M, Demirci G, Muti A, Ulukaya E, Sennaroglu A, Yagci Acar H: The improved killing of both androgen-dependent and independent prostate cancer cells by etoposide loaded SPIONs coupled with NIR irradiation. Biomater Sci 2022, 10(14): 3951-3962.
- Dai L, Wei D, Zhang J, Shen T, Zhao Y, Liang J, Ma W, Zhang L, Liu Q, Zheng Y: Aptamer-conjugated mesoporous polydopamine for docetaxel targeted delivery and synergistic photothermal therapy of prostate cancer. Cell Prolif 2021, 54(11): e13130.
- SreeHarsha N, Maheshwari R, Al-Dhubiab BE, Tekade M, Sharma MC, Venugopala KN, Tekade RK, Alzahrani AM: Graphene-based hybrid nanoparticle of doxorubicin for cancer chemotherapy. Int J Nanomedicine 2019, 14: 7419-7429.
- Lin W, Li C, Xu N, Watanabe M, Xue R, Xu A, Araki M, Sun R, Liu C, Nasu Y, et al: Dual-Functional PLGA Nanoparticles Co-Loaded with Indocyanine Green and Resiquimod for Prostate Cancer Treatment. Int J Nanomedicine 2021, 16: 2775-2787.
- Liu J, Song Y, Wang Y, Han M, Wang C, Yan F: Cyclodextrin-Functionalized Gold Nanorods Loaded with Meclofenamic Acid for Improving N(6)-Methyladenosine-Mediated Second Near-Infrared Photothermal Immunotherapy. ACS Appl Mater Interfaces 2022, 14(36): 40612-40623.
- Huang X, Chen L, Lin Y, Tou KI, Cai H, Jin H, Lin W, Zhang J, Cai J, Zhou H, et al: Tumor targeting and penetrating biomimetic mesoporous polydopamine nanoparticles facilitate photothermal killing and autophagy blocking for synergistic tumor ablation. Acta Biomater 2021, 136: 456-472.
- Qiang L, Cai Z, Jiang W, Liu J, Tai Z, Li G, Gong C, Gao S, Gao Y: A novel macrophage-mediated biomimetic delivery system with NIR-triggered release for prostate cancer therapy. J Nanobiotechnology 2019, 17(1): 83.
- Liu L, Yang S, Zheng Z, Li Q, Liu C, Hu D, Liu Z, Zhang X, Zhang R, Gao D: Biomimetic Theranostic Agents with Superior NIR-II Photoacoustic and Magnetic Resonance Imaging Performance for Targeted Photothermal Therapy of Prostate Cancer. Pharmaceutics 2023, 15(6): 1617.
- Huang L, Xu C, Xu P, Qin Y, Chen M, Feng Q, Pan J, Cheng Q, Liang F, Wen X, et al: Intelligent Photosensitive Mesenchymal Stem Cells and Cell-Derived Microvesicles for Photothermal Therapy of Prostate Cancer. Nanotheranostics 2019, 3(1): 41-53.
- Thapa RK, Soe ZC, Ou W, Poudel K, Jeong JH, Jin SG, Ku SK, Choi HG, Lee YM, Yong CS, et al: Palladium nanoparticle-decorated 2-D graphene oxide for effective photodynamic and photothermal therapy of prostate solid tumors. Colloids Surf B Biointerfaces 2018, 169: 429-437.
- Wang Q, Zhang X, Sun Y, Wang L, Ding L, Zhu WH, Di W, Duan YR: Gold-caged copolymer nanoparticles as multimodal synergistic photodynamic/photothermal/chemotherapy platform against lethality androgen-resistant prostate cancer. Biomaterials 2019, 212: 73-86.
- Tan H, Hou N, Liu Y, Liu B, Cao W, Zheng D, Li W, Liu Y, Xu B, Wang Z, et al: CD133 antibody targeted delivery of gold nanostars loading IR820 and docetaxel for multimodal imaging and near-infrared photodynamic/photothermal/chemotherapy against castration resistant prostate cancer. Nanomedicine 2020, 27: 102192.
- Hu J, Luo H, Qu Q, Liao X, Huang C, Chen J, Cai Z, Bao Y, Chen G, Li B, et al: Cell Membrane-Inspired Polymeric Vesicles for Combined Photothermal and Photodynamic Prostate Cancer Therapy. ACS Appl Mater Interfaces 2020, 12(38): 42511-42520.
- Sarbadhikary P, George BP, Abrahamse H: Recent Advances in Photosensitizers as Multifunctional Theranostic Agents for Imaging-Guided Photodynamic Therapy of Cancer. Theranostics 2021, 11(18): 9054-9088.
- Pham TC, Nguyen VN, Choi Y, Lee S, Yoon J: Recent Strategies to Develop Innovative Photosensitizers for Enhanced Photodynamic Therapy. Chem Rev 2021, 121(21): 13454-13619.
- Gallardo-Villagrán M, Paulus L, Charissoux JL, Sutour S, Vergne-Salle P, Leger DY, Liagre B, Therrien B: Evaluation of Ruthenium-Based Assemblies as Carriers of Photosensitizers to Treat Rheumatoid Arthritis by Photodynamic Therapy. Pharmaceutics 2021, 13(12): 2104.
- Nkune NW, Matlou GG, Abrahamse H: Photodynamic Therapy Efficacy of Novel Zinc Phthalocyanine Tetra Sodium 2-Mercaptoacetate Combined with Cannabidiol on Metastatic Melanoma. Pharmaceutics 2022, 14(11): 2418.
- Dandash F, Leger DY, Diab-Assaf M, Sol V, Liagre B: Porphyrin/Chlorin Derivatives as Promising Molecules for Therapy of Colorectal Cancer. Molecules 2021, 26(23): 7268.
- Riley RS, Day ES: Gold nanoparticle-mediated photothermal therapy: applications and opportunities for multimodal cancer treatment. Wiley Interdiscip Rev Nanomed Nanobiotechnol 2017, 9(4): 10.
- Pinho S, Coelho JMP, Gaspar MM, Reis CP: Advances in localized prostate cancer: A special focus on photothermal therapy. Eur J Pharmacol 2024, 983: 176982.
- Overchuk M, Weersink RA, Wilson BC, Zheng G: Photodynamic and Photothermal Therapies: Synergy Opportunities for Nanomedicine. ACS Nano 2023, 17(9): 7979-8003.
Cite this article: Usman A: Advances in Illuminating Prostate Cancer with Emerging Phototherapies. Ann Urol Oncol 2025, 8(1): 21-29. https://doi.org/10.32948/auo.2025.01.29
Annals of urologic oncology
p-ISSN: 2617-7765, e-ISSN: 2617-7773
 Copyright © Ann Urol Oncol. This work is licensed under a Creative Commons Attribution-NonCommercial-No Derivatives 4.0 International (CC BY-NC-ND 4.0) License.
Copyright © Ann Urol Oncol. This work is licensed under a Creative Commons Attribution-NonCommercial-No Derivatives 4.0 International (CC BY-NC-ND 4.0) License.